Answer of September 2014
Clincial History:
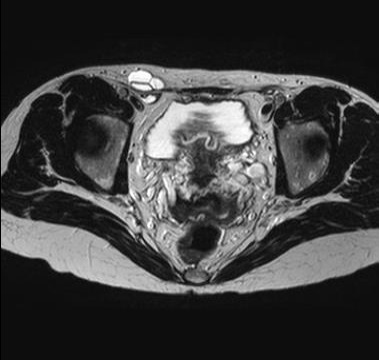
A 40 year-old female presented with right groin swelling with occasional pain. Physical examination revealed smooth swelling in the right inguinal region which was tense but not tender. Ultrasound (USG) and Magnetic Resonance Imaging (MRI) of pelvis were performed.




Diagnosis:
Hydrocele of Canal of Nuck
Discussion:
The canal of Nuck was first described by the Dutch anatomist Anton Nuck in 1691. The processus vaginalis within the inguinal canal in women is therefore called the canal of Nuck. It an abnormal evagination of parietal peritoneum extending anterior to the round ligament of the uterus into the labium majus. Failure of complete obliteration of this canal results in either an inguinal hernia or a hydrocele.
A hydrocele of the canal of Nuck is a rare condition in female, and generally manifests as a painless swelling in the inguinal area and labium in adolescent age groups. Hydroceles can be painful and cause a red swelling extending to the labium majus in case of infection. The size of the lesion is usually small, with average length about 3cm. Herniation of urinary bladder, ovary and fallopian tubes into the canal of Nuck is rarely reported. Unlike inguinal hernia, there is no change on Valsalva maneuver and absence of cough impulse.
Ultrasound is the preferred investigation due to the superficiality of the lesion, which is readily visualized with a high frequency transducer. The lesion is typically cystic, superficially and medially to the pubic bone at the level of the superficial inguinal ring. No communication with the peritoneum should be visible. Septations within the lesion are common, as seen in our case. Some authors suggested that sausage-shaped cystic lesion extending along the route of the round ligament, or comma-shaped with surface beak representing a continuation of the peritoneal cavity through the inguinal canal are characteristic.
MR findings of a hydrocele of the canal of Nuck include a thin-walled tense cystic mass in inguinal area. The proximal part of the lesion extends in the peritoneal cavity along the route of the round ligament, where the distal part is blunt and extending towards the labium majus. The wall of the hydrocele may show mild contrast enhancement, and if infected, the wall can be thick and markedly enhanced.
The differential diagnoses for inguinal masses in young female and children also include indirect inguinal hernia, lymphadenopathy, abscess, Bartholin’s cyst, malignant and benign tumors (lipoma, leiomyoma, sarcoma).
Complications of the hydrocele of the canal of Nuck are infection and haemorrhage.
Regarding the management, hydroceles can be treated surgically. However, some surgeons prefer conservative treatment. In case of infection, antibiotic therapy should be started.