Answer of March 2014
Clinical History:
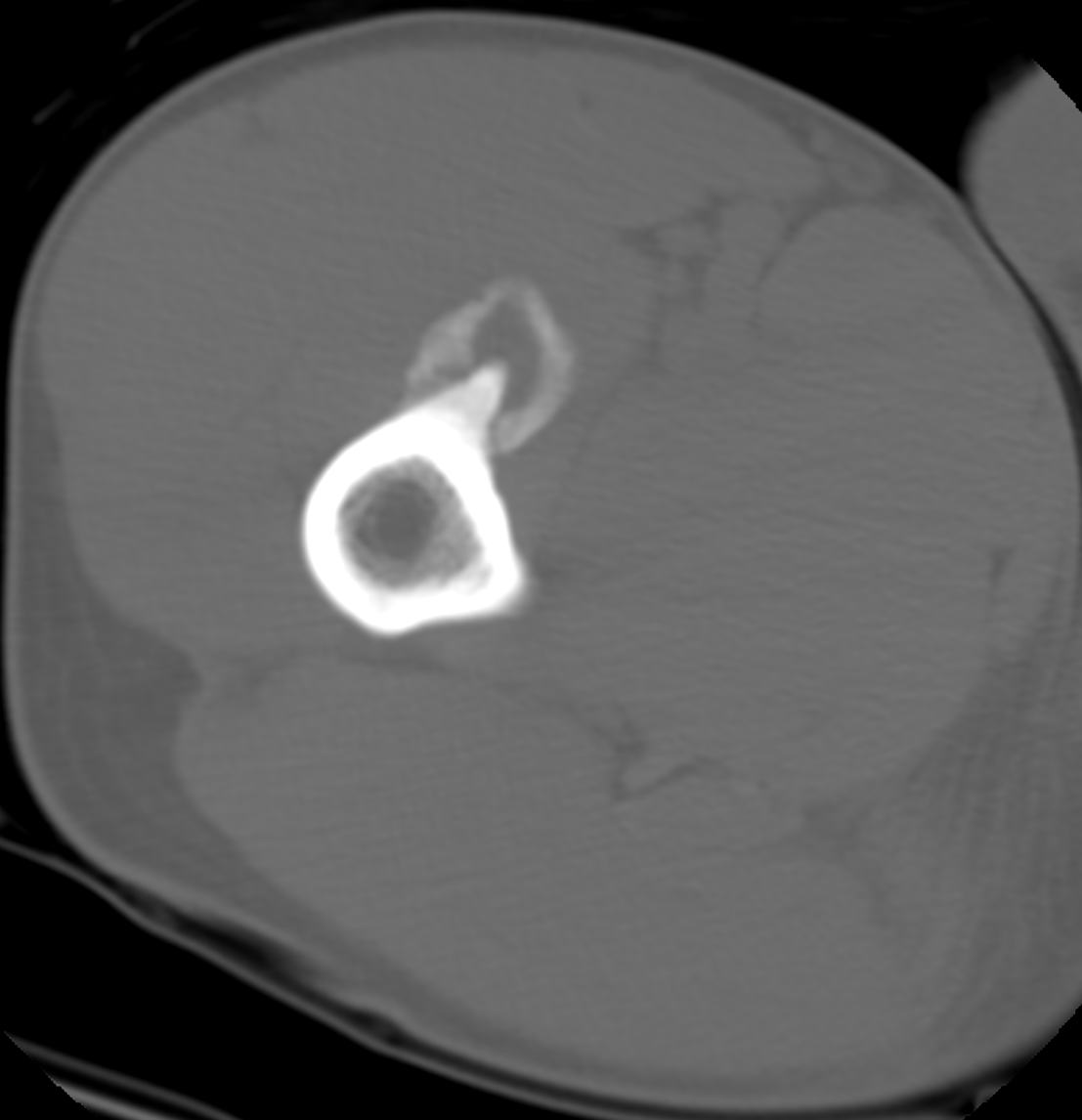
A 45-year-old male badminton coach, otherwise well, presented with a right proximal anterior thigh pain for 1 year. Pain intensity and swelling had increased during the month prior to presentation. There was no history of any specific hip or thigh injury. Plain radiography and CT of right thigh were performed (2 images: XR and axial CT of right upper femur).

Diagnosis:
Myositis ossificans related to femur traction spur
Discussion:
Radiography revealed a large traction spur arising from the anteromedial aspect of the proximal femur (Figure 1). There was a rim of peripheral calcification surrounding this bony spur (Figure 1). Computed tomography (CT) revealed that the traction spur was at the femoral origin of the vastus intermedialis and medialis muscles (Figure 2). There was a soft tissue lesion with peripheral calcification surrounding the prominent traction femoral spur within the proximal vastus intermedialis and medialis (Figure 2). There is no cortical erosion or intramedullary extension. The provisional diagnosis was myositis ossificans traumatica with a traction spur and conservative treatment was given. The symptoms resolved spontaneously in one month with restriction of badminton activity. Overall clinical and radiological features were compatible with myositis ossificans of vastus muscle caused by femoral traction spur (from the femoral attachment vastus muscles) due to overuse.
Myositis ossificanstraumatica (MOT) is also called localized myositis ossificans, myositis ossificans circumscripta (MOC) or post-traumatic myositis ossificans (1). This accounts for 75% of myositis ossificans and is much more common than non-traumatic myositis ossificans which is usually due to systemic disease (such as chronic infection, poliomyelitis or hemophilia) (1). Most (60 – 75 %) cases of myositis ossificans traumatica have a history of trauma which induces a proliferative mesenchymal response to muscle injury (1). It is postulated that the remaining patients may also have had minor trauma that cannot be recalled. Trauma may be acute and isolated or chronic and repetitive, often associated with sports injuries. The occurrence of MOT related to overuse is rare. Only three case reports relate the development of MOT to overuse (2). Two developed myositis ossificans in the thigh muscles after running (2) while one sustained myositis ossificans of the triceps muscle from swimming training (2). Overuse may induce microscopic muscle injury inducing an inflammatory reaction which encourages the differentiation of fibroblasts into osteoblasts and developmental of MOT (2).
Traction spur mainly occur in the femur at the attachment of strong thigh muscles. The large femoral spur in our case is related to chronic traction of the thigh musculature during badminton which requires frequent forward stepping with the knee in flexion and quadriceps muscle contraction while hitting. The origin of the vastus muscles takes most of this strain with changes only in the right femur. The large traction spur indents the adjacent vastus muscle leading to muscle injury and the development of myositis ossificans. The occurrence of myositis ossificans due to traction spur has not been reported.