Answer of January 2024
For completion of the online quiz, please visit the eHKAM LMS website.
Clinical History:
53 years old man, who works as a cook, presented with acute onset of bilateral hearing loss, vomiting and fever for one day. On examination, he had positive Kernig’s sign and Brudzinski's sign. Plain CT Brain was unremarkable. White cell count was raised. Lumbar puncture was performed revealing raised leukocytes with positive gram stain - gram positive cocci in chains. He was treated empirically as bacterial meningitis but had persistent hearing impairment. CT Petrous Temporal Bones and MRI Internal Acoustic Meatus were performed.

CT Petrous Temporal Bones
Axial T1-Weighted Image of MRI Internal Acoustic Meatus
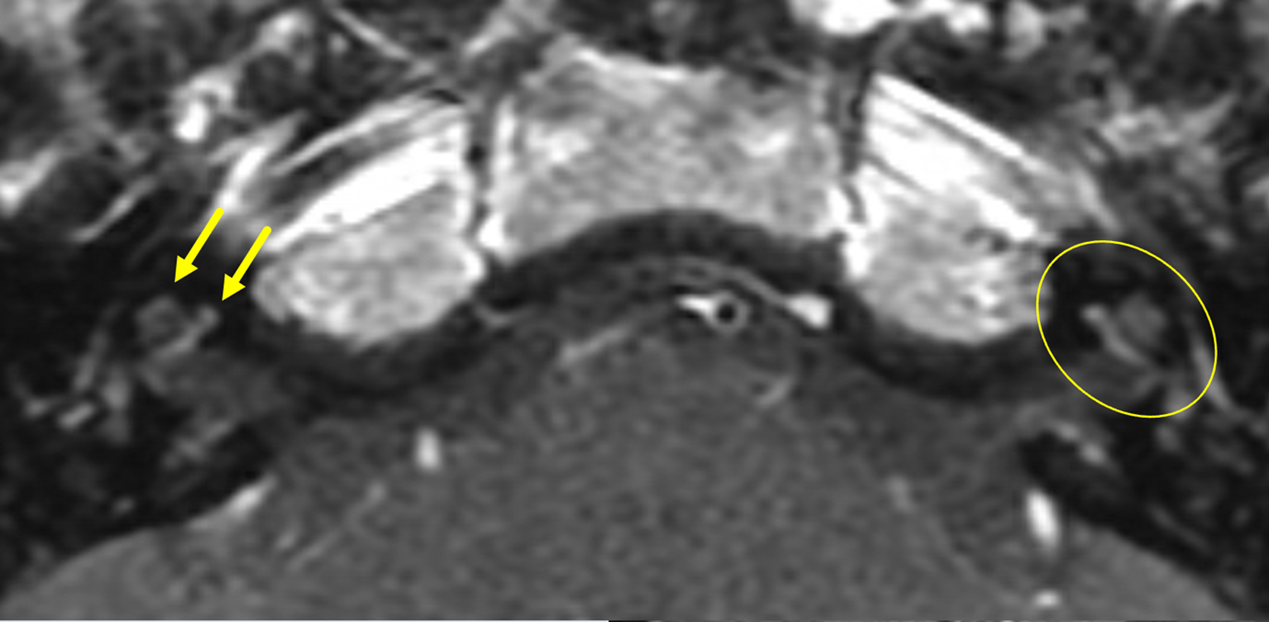
Axial T2-Weighted Image of MRI Internal Acoustic Meatus

Axial Contrast-Enhanced T1-Weighted Image of MRI Internal Acoustic Meatus
DIAGNOSIS
Streptococcus suis meningitis with bilateral hemorrhagic labyrinthitis
DISCUSSION
Streptococcus Suis infection is an uncommon zoonotic disease and is listed as one of the fifty-three notifiable infectious diseases in Hong Kong. It is usually associated with an occupational history of handling diseased pigs or raw pork e.g. butchers or cooks.
The most common presentation of Streptococcus Suis infection is meningitis. Patients commonly present with symptoms such as headache, vomiting, fever and neck stiffness. Over half of the patients also have hearing loss which is bilateral, severe and permanent. This is due to concomitant labyrinthitis which is caused by direct bacterial invasion from subarachnoid space into the inner ear through cochlear duct.
MRI is useful in detecting labyrinthitis changes
and confirming diagnosis. For our case, there is loss of normal T2
hyperintensity within bilateral vestibulocochlear apparatuses and associated abnormal
enhancement within both cochlea suggestive of labyrinthitis. There is also
presence of slight T1 hyperintensity at the basal turns of cochlea and
vestibules on the T1W pre contrast images suggestive of haemorrhagic component.
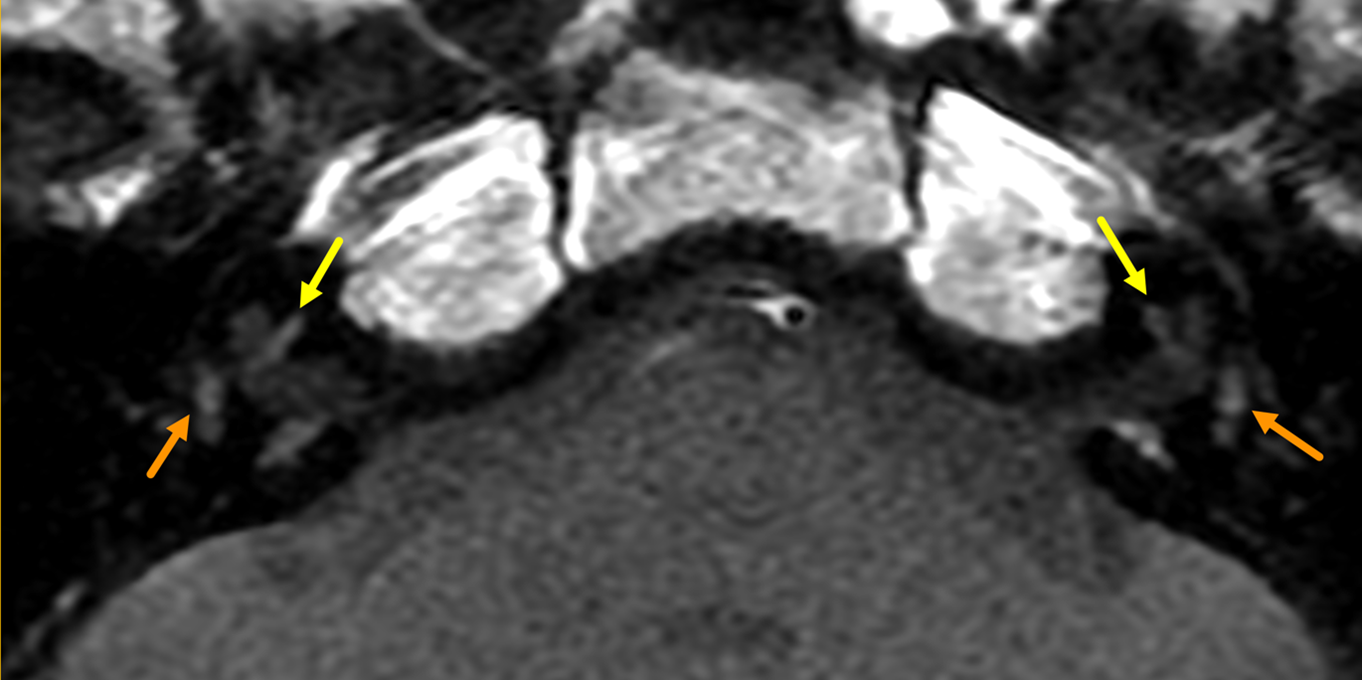
Axial T1-Weighted Image of MRI Internal Acoustic Meatus - T1 Hyperintensity at the Basal Turns of Cochlea (Yellow Arrows) and Vestibules (Orange Arrows)
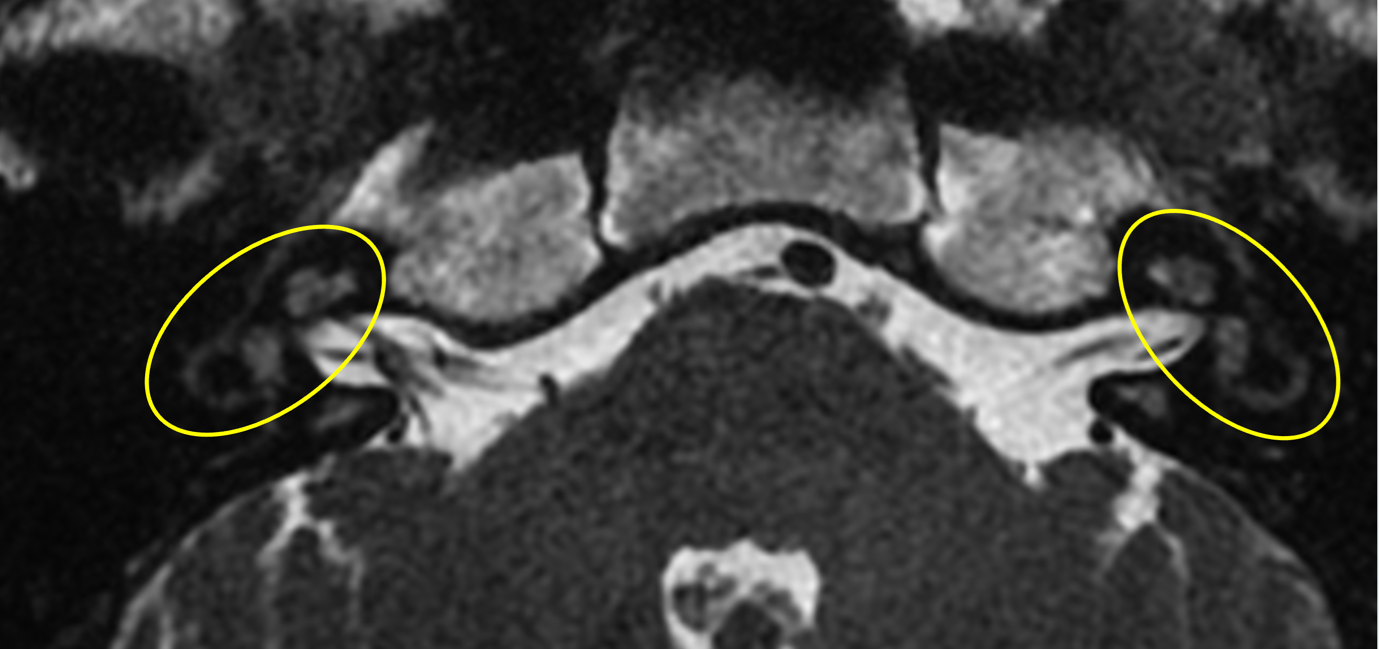
Axial T2-Weighted Image of MRI Internal Acoustic Meatus – Loss of T2 Hyperintensity within Bilateral Vestibulocochlear Apparatuses (Circled in Yellow)

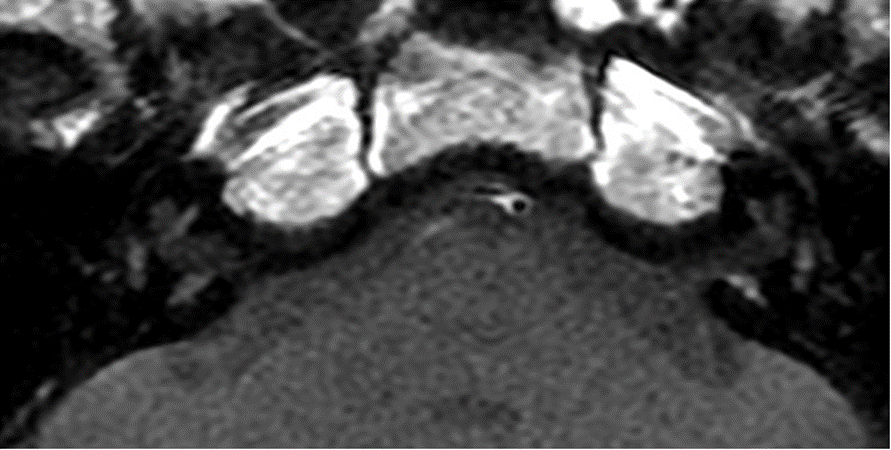
Normal Axial T2-Weighted Image of MRI Internal Acoustic Meatus for Comparison
Axial Contrast-Enhanced T1-Weighted Image of MRI Internal Acoustic Meatus
– Contrast Enhancement of the Right Cochlea involving the Apical and Basal Turns (Yellow Arrows)
– Contrast Enhancement of the Left Cochlea involving the Apical, Middle and Basal Turns (Circled in Yellow)
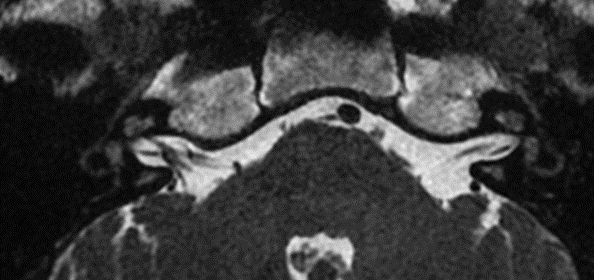
CT Petrous Temporal Bones in our case also showed small foci of fluid opacification near bilateral oval windows which were shown to be pus intra-operatively. Otherwise, mastoid air cells were clear with unremarkable CT appearances of the vestibulocochlear apparatus.
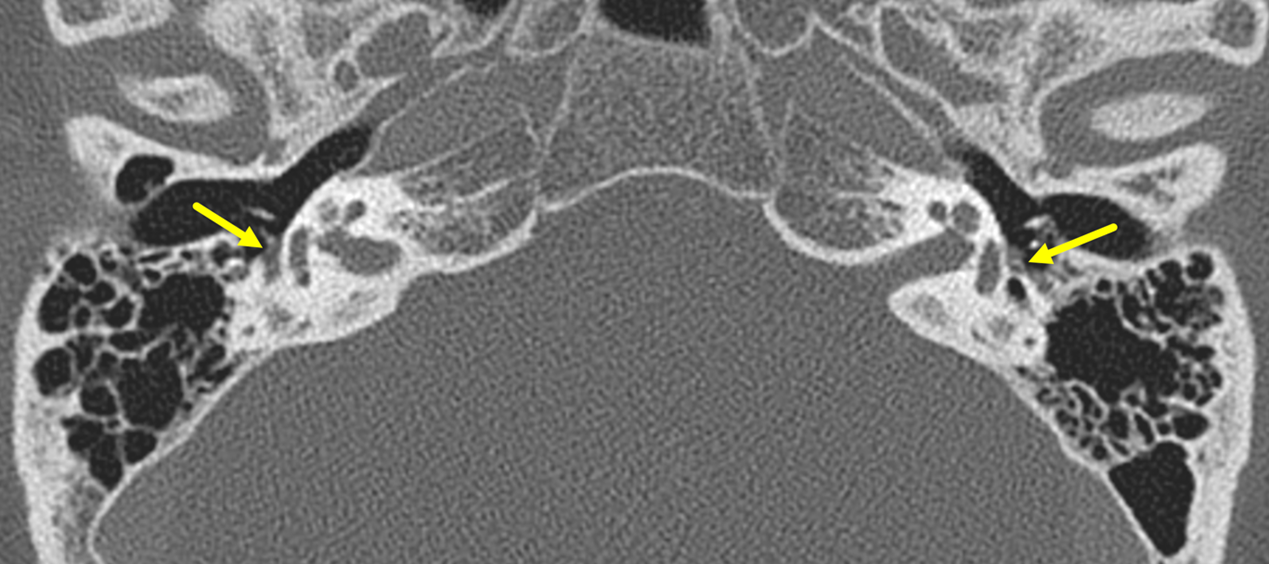
CT Petrous Temporal Bones – Fluid Opacification near Bilateral Oval Windows (Yellow Arrows)
The mainstay of treatment is early intravenous administration of Penicillin with a usual duration of two to four weeks. Relapse may also be seen in some patients and can be treated with a prolonged course of antibiotics. The use of corticosteroids remains controversial with one randomized controlled trial in Vietnam showing significant reduction in hearing loss with dexamethasone while other case series showed inconsistent results. Cochlear implantation can also potentially improve patient’s hearing but needs to be placed before secondary cochlear ossification occurs. CT Petrous Temporal Bones and MRI Internal Acoustic Meatus are useful in these cases for the assessment of the inner ear for underlying anatomy or associated abnormalities, middle ear for concomitant pathologies and to rule out conditions which precludes surgery e.g. aplastic/hypoplastic cochlear nerve.