Answer of October 2023
For completion of the online quiz, please visit the eHKAM LMS website.
Clinical History:
A 72-year-old lady presenting with shock.

CT Abdomen with precontrast

CT Abdomen with postcontrast (Arterial phase)

CT Abdomen with post-contrast (PVphase)
DIAGNOSIS
Iatrogenic liver laceration
IMAGING FINDING
CT Abdomen with precontrast - Pericardiocentesis catheter transverse the prehepatic space. Hemopericardium and hemoperitoneum is noted.
CT Abdomen with postcontrast (Arterial phase) - Active contrast extravasation anterior to the left liver lobe in the prehepatic space.
CT Abdomen with post-contrast (PV phase) - Contrast pooling during portovenous phase.
DISCUSSION
The patient was diagnosed to have iatrogenic liver laceration due to subxiphoid approach of pericardiocentesis. Patient was in shock and was given colloid and blood products transfusion but the patient was not responsive. Subsequent angiograms showed contrast extravasation and pooling from a S3 small branch.

Superselective catheterization of S3 segmental artery, and embolization was performed with EgGel. Achieved successful devascularization of bleeder and stasis in S3 artery.
Table 1 describes the three possible approaches for draining pericardial effusions. In general, the anatomic approach to PC is dictated by the location of the largest collection of fluid and the ease of percutaneous access.
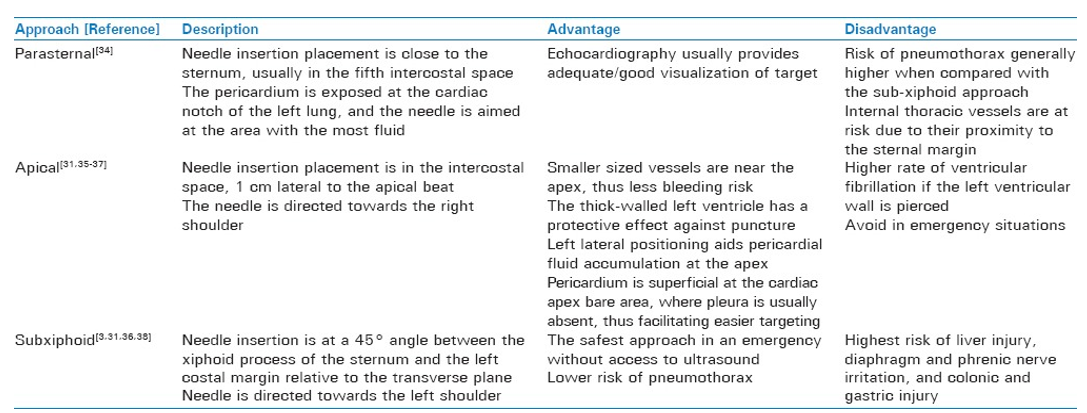
Table 1
Subxiphoid approach has higher rates of accidental infradiaphragmatic organ injury including liver laceration as in our case. Alternative parasternal and apical approaches also have their specific risks. The literature describes hemoperitoneum and hemorrhagic peritonitis following the subxiphoid approach (3,4).