Answer of August 2023
For completion of the online quiz, please visit the eHKAM LMS website.
Clinical History:
A 53-year-old man with history of depression with psychotic symptoms, presented to Emergency Department acutely with abdominal pain, shock and hemoglobin drop.

Fig.1 Contrast CT
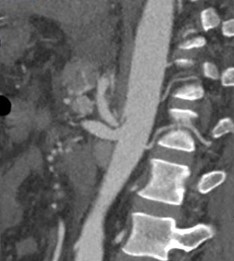

Fig.2 and 3 Reconstruction of CT angiogram


Fig.4 and 5 Digital subtraction angiogram - superior mesenteric artery run

Fig. 6 Digital subtraction angiogram – selective run at inferior pancreaticoduodenal artery
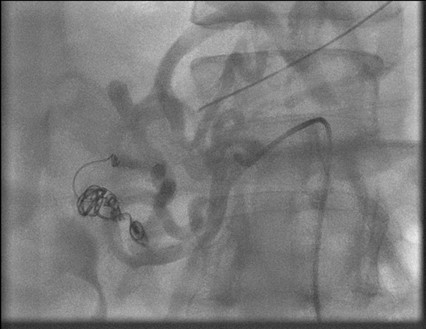
Fig .7 Digital subtraction angiogram – post-embolization superior mesenteric artery run
DIAGNOSIS
Median arcuate ligament syndrome, complicated with anterior pancreaticoduodenal artery pseudoaneurysm and hemorrhage
IMAGE FINDINGS
CT angiogram
Large amount of hemoperitoneum. A large acute retroperitoneal hematoma adjacent to second part of duodenum. Multiple prominent arteries adjacent to the acute hematoma, corresponding to hypertrophied pancreaticoduodenal arcade. No active contrast extravasation. Severe stenosis at celiac trunk origin, with superior indentation, by extrinsic compression. No pseudoaneurysm.
Digital subtraction angiogram
Difficult cannulation of celiac trunk despite repeated attempts. Successful cannulation of superior mesenteric artery. Prominent pancreaticoduodenal arcade, and retrograde opacification of celiac trunk. Focal dilatation at mid portion of anterior pancreaticoduodenal artery represents pseudoaneurysm. Selective embolization with coils at site of pseudoaneurysm.
Preserved retrograde opacification of celiac trunk demonstrated after embolization.
DISCUSSION
Median arcuate ligament syndrome, also known as Dunbar syndrome, is uncommon condition. The pathophysiology is that the median arcuate ligament compresses on celiac trunk causing vascular insufficiency, with or without symptoms such as dyspepsia, weight loss or rarely bowel ischemia.
A study showed that, in individuals without symptoms suggestive of MALS, 13-50% were found to have MALS anatomy. (1) Only 1% of subjects with anatomical compression showed symptoms.
This condition predominantly affects young female, with ratio of 4:1. (2)
Anatomical delineation by CT or MR angiography to show superior extrinsic compression of celiac trunk, with post-stenotic dilatation and hook-like configuration, are suggestive, while clinical evaluation of symptoms is needed.
Digital subtraction angiogram is reserved for interventional purpose, such as stenting or embolization.
Complications like collateral development, and pseudoaneurysm with hemorrhage are rare.
Decompression of the celiac trunk is usually done by division of the ligament, either or laparotomy or laparoscopy. Angioplasty with stenting can be an alternative modality. (2)
For median arcuate ligament syndrome, cannulation of celiac trunk during DSA will be difficult. Embolization of collaterals from superior mesenteric artery non-selectively may lead to celiac territory ischemia.