Answer of June 2023
For completion of the online quiz, please visit the eHKAM LMS website or HKAM iCMECPD website.
Clinical History:
60 year old lady with bilateral hip pain for years. She complains of increasing left hip pain with no preceding trauma recalled.

X-ray pelvis

X-ray left femur

X-ray left femur

Plain CT left femur
Bone window
Coronal
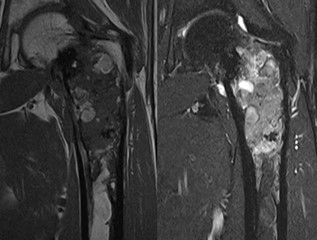
MRI left femur
T1 (left)
T2 (right)
DIAGNOSIS
Fibrous dysplasia
IMAGING FINDINGS
- Expansile mixed sclerotic and radiolucent lesions in both proximal femurs, with ground-glass
appearance and endosteal scalloping.
- Pathological fracture at left femoral neck.
- Heterogeneous T1 and T2 signals with hypo-, iso- and hyperintense components.
DISCUSSION
Fibrous dysplasia is a sporadic fibro-osseous proliferative disease where normal marrow is replaced by immature bone and fibrous tissue. While a benign process, it may be complicated by pathological fracture and rarely (<1%) malignant degeneration. It is commonly monostotic but can also present in a polyostotic form. Associated conditions include McCune-Albright syndrome, an endocrinopathy consisting of precocious puberty and café au lait spots, and Mazabraud syndrome, a combination with soft-tissue myxomas.
Lesions are often incidentally found and asymptomatic, although they could cause pain or other symptoms due to mass effect. They frequently involve the ribs, limbs and craniofacial bones. In the polyostotic form, the proximal femurs are most commonly involved. The spine is a documented but more uncommon site of involvement especially in the absence of disease elsewhere.
General imaging features are of an intramedullary expansile lesion with well-defined borders. Endosteal scalloping and cortical thinning may be seen but a smooth contour is maintained. It could appear lucent, sclerotic or mixed. Typical description of a ground-glass matrix can be present in varying degrees. Bowing deformities can be seen in the long bones, and in the femoral neck specifically, the ‘Shepherd crook deformity’ describes a resultant coxa varus angulation. Diagnosis can be made based on clinical and radiological features alone if characteristic.
Fibrous dysplasia on 99m-Tc-MDP bone scan demonstrates increased tracer uptake and could remain metabolically active. While bone scans are sensitive in detection and assessing extent of disease, follow up bone scan is generally not recommended. They also show variable FDG uptake which may mimic malignancy.
MRI findings are also non-specific with variable T2 signal and heterogeneous enhancement.
Follow up with serial radiographs is usually preferred. Findings concerning of malignant change include cortical destruction and presence of soft tissue mass.
In our case, this patient was subsequently
referred to an orthopaedic tumour center for biopsy to rule out malignant
transformation before arrangement of left femur fixation. Results were
compatible with fibrous dysplasia with no malignancy detected.