Answer of April 2023
For completion of the online quiz, please visit the eHKAM LMS website or HKAM iCMECPD website.
Clinical History:
A 55-year-old patient has past history of nasopharyngeal carcinoma treated with radiotherapy 10 years ago. He presents with increasing pain and numbness at left sided face.
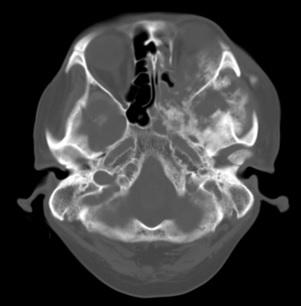
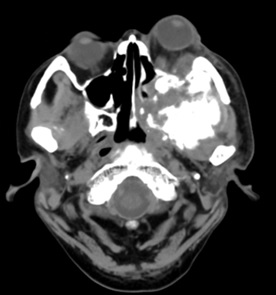
CT brain (plain)


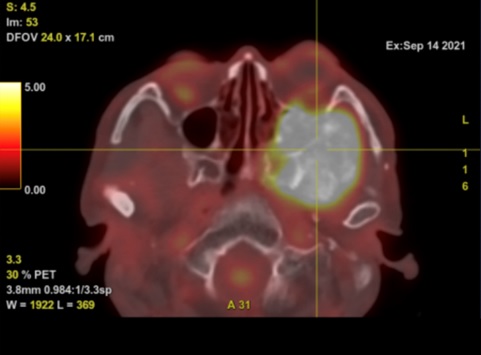
PET-CT (plain)
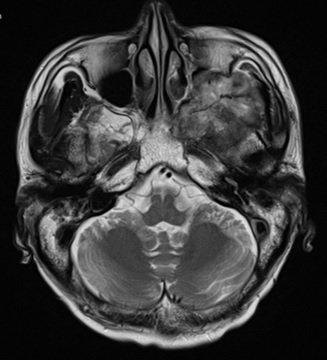
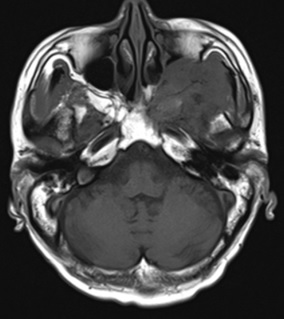
MRI brain (plain and contrast)
T2W
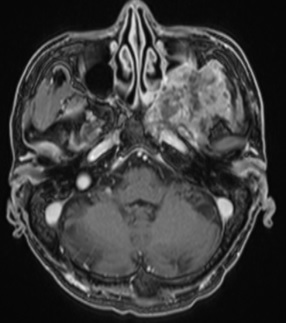
T1W image (pre- and post-contrast)
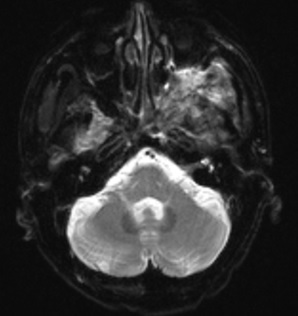
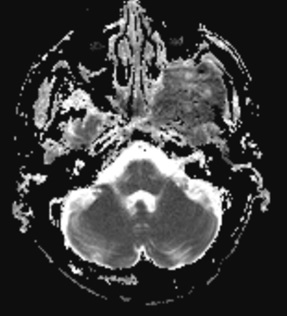
DWI with ADC map
DIAGNOSIS
Radiation-induced osteosarcoma of the skull base
IMAGING FINDINGS
CT brain (plain):
- - A large mass with ossified matrix and adjacent soft tissue densities is noted in the left sided skull base with involvement of the left middle cranial fossa, extra-and intra-conal spaces of left orbit, left infratemporal fossa, left maxillary, sphenoid and posterior ethmoidal sinuses, left ptergomaxillary fissure and left pterygopalatine fossa, and left sided nasal cavity. Associated left sided proptosis is noted. Bony destruction of left sided clivus, left pterygoid and left sphenoid wing is evident.
PET-CT (plain):
- - The left sided skull base mass shows very high FDG avidity.
MRI brain (plain and contrast):
- - The left sided skull base mass shows heterogeneous predominantly T1W hypointense and T2W hyperintense signals. Associated heterogeneous contrast enhancement and restricted diffusion are noted. Involvement of the left infratemporal fossa, left maxillary sinus, left ptergomaxillary fissure and left pterygopalatine fossa is evident. Bony destruction of left sided clivus, left pterygoid and left sphenoid wing is seen.
DISCUSSION
Nasopharyngeal carcinoma (NPC) is one of the commonest malignancies in Asia, especially China. Radiation therapy is the initial treatment for these patients. However, it may potentially lead to the development of secondary malignancies. Radiation-induced tumor is defined as tumor which develops after a post-irradiation latent period within the site of irradiation. Although it is rare, this possibility should be considered in any patients who have received radiation therapy.
The target volumes of radiotherapy for nasopharyngeal carcinoma include the skull base, as well as the maxilla, mandible and pterygoid bone. Therefore, radiation-induced tumors, such as radiation-induced sarcomas (RISs), can arise in these sites post-irradiation as one of the late complications. According to the Cahan’s criteria, RIS was defined as: 1) a second neoplasm occurs in the field of previous irradiation; 2) the sarcoma of the irradiated lesion is histologically different from that of the primary cancer; 3) the incubation period from irradiation to sarcoma development is more than 5 years; 4) the sarcoma must be proven histologically. In these patients, the latent period for development of secondary tumors following radiation therapy is usually around 5-30 years.
The incidence of radiation-induced osteosarcoma (RIOS) ranges from 0.01% to 0.03% of all irradiated patients and accounts for 5.5% of all osteosarcomas. Histologically, RIOS is characterized by more aggressive features than primary osteosarcoma. RIOS in the head and neck region poses a particular challenge, especially when involving the skull base. These lesions are usually difficult to excise completely, because they may abut or involve important neurovascular structures, and they have a high propensity to recur. Follow-up within the radiation field by CT and MRI and a recognition of the expected latency period may assist in making early diagnosis. From the radiological perspective, there are no particular imaging findings to differentiate RIOS from non-RIOS. The distinction therefore relies mainly on clinical history and location within the field of previous irradiation. Complete surgical excision is the treatment of choice for RIOS, although this can be difficult in tumors involving the skull base. Palliative chemotherapy should be considered in patients with unresectable disease.