Answer of February 2023
For completion of the online quiz, please visit the eHKAM LMS website or HKAM iCMECPD website.
Clinical History:
A 68-year-old lady presented with dysphagia and vomiting.
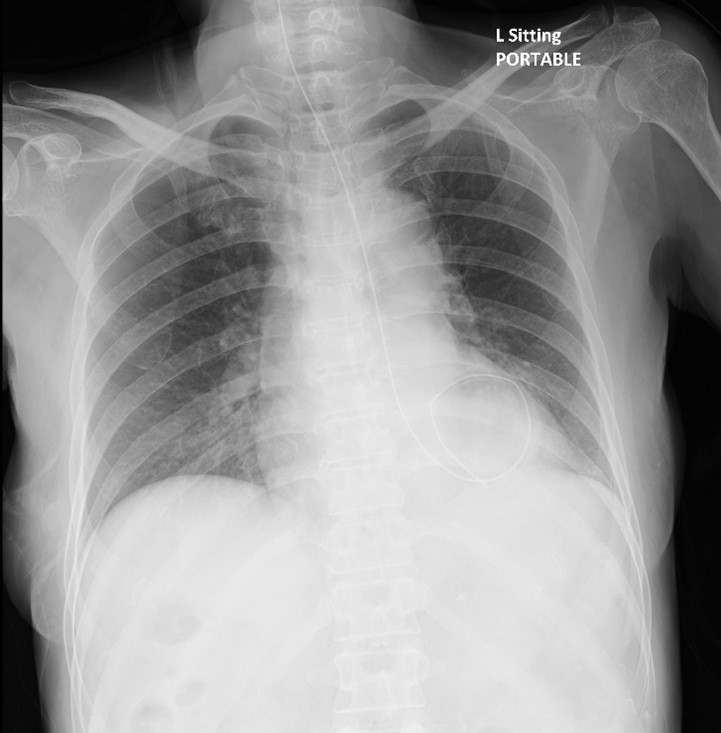
CXR images (pre- and post-adjustment of feeding tube position):

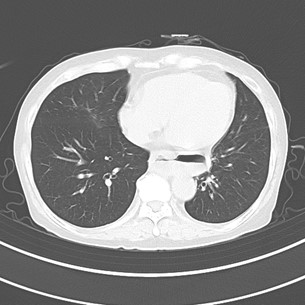
CT images (axial, axial lung window, coronal, sagittalx2):




DIAGNOSIS
Pulsion epiphrenic esophageal diverticulum.
IMAGING FINDINGS
CXR: The first CXR shows increased opacity in the left retrocardiac region which silhouettes the medial aspect of the left hemidiaphragm. There is coiling of the distal part of the feeding tube in the left retrocardiac region. The second CXR shows a well-defined opacity air-fluid level in the left retrocardiac region. The feeding tube is in-situ in the second CXR.
CT: The thoracic esophagus is dilated with air-fluid level. There is a long segment of circumferential mural thickening of the distal esophagus. A focal outpouching with air-fluid level is seen arising from the left-sided distal esophageal wall. The adjacent lung parenchyma is unremarkable.
DISCUSSION
The differential diagnoses of a retrocardiac opacity with air-fluid level shown in CXR include hiatus hernia, esophageal diverticulum, lung abscess, Bochdalek hernia etc. The first CXR shows the coiling of the distal part of the feeding tube in the left retrocardiac region, suggesting that the retrocardiac lesion has direct communication with the esophagus and is likely gastrointestinal tract in origin. CT shows a focal outpouching arising from the esophageal wall, compatible with the diagnosis of esophageal diverticulum. Pulsion esophageal diverticula are commonly located in the distal third of the esophagus and appear as well-defined roundish outpouching. They are formed due to increased intraluminal esophageal pressure from underlying esophageal dysmotility. They are false diverticula as only the mucosa and submucosa herniate through the muscular layer. Traction esophageal diverticula are commonly located in the middle third of the esophagus, and usually have a triangular configuration due to negative mass effect from adjacent lung parenchymal fibrosis. They are true diverticula and contain all of the esophageal wall layers. The CT study shows that the outpouching is well-defined and roundish in shape, and there is no adjacent lung parenchymal change. Features are suggestive of pulsion esophageal diverticulum. Besides, in the CT, the thoracic esophagus is dilated with air-fluid level, and a long segment of circumferential mural thickening of the esophagus is seen. This may imply underlying diffuse esophageal spasm, which could be the cause of the formation of pulsion esophageal diverticulum in this case.