Answer of November 2022
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 67-year-old lady complains of a 2-week history of a hard left pre-auricular mass. Patient was otherwise in good health.
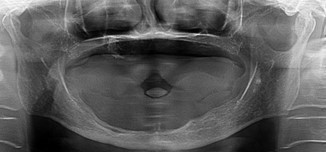
OPG
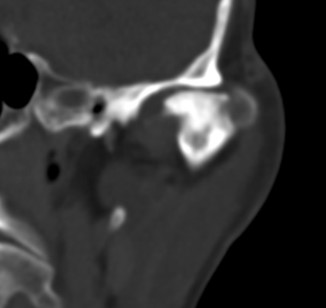
CT with contrast - coronal
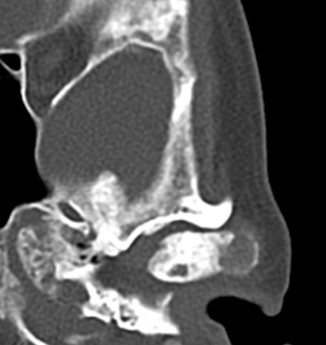
CT with contrast - axial
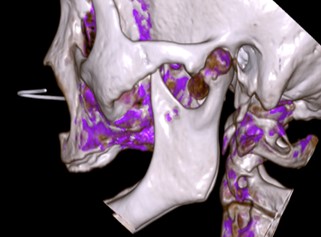
Dual Source Energy CT
DISCUSSION:
Chondroma is a benign tumor of mature hyaline cartilage of mesenchymal origin. Based on their location, chondromas can be classified as (1) enchondromas that are located in the medullary cavity of the bony skeleton; (2) juxtacortical or periosteal chondromas that originate adjacent to the periosteum below the cortical surface; and (3) extra-skeletal or soft tissue chondromas, which have been reported in the tongue and buccal mucosa.
Chondromas have no specific sex predilection and are usually discovered in the third and fourth decade of life.Most chondromas are asymptomatic. Chondromas involving the TMJ may often go undetected or be clinically confused with joint dysfunction, owing to its rarity. This condition may be associated with a variety of symptoms ranging from clicking, limited mouth opening, deviation, mild symptoms to episodes of condylar dislocation. They are almost always slow growing in nature.
The orthopantomogram (OPG) showed a left sided enlarged condyle of the mandible. The computed tomography scan confirmed the left sided condylar mass.
Radiographically, chondromas are predominantly radiolucent, irregular masses. They may have some calcified foci ranging from powder like to dense aggregates.
The microscopic distinction between chondroma and low-grade chondrosarcoma may at times be very difficult. The distinction between the two becomes even more ambiguous owing to their common radiological and clinical findings. So in such cases careful histological examination is essential to take note of cellular atypia, change in nuclear-cytoplasm ratio, increased cellularity or any other dysplastic features. The incidence of malignant transformation in cases of multiple chondromas is reported to be as high as 20-33%.
Surgical resection is the treatment of choice for the chondroma of the mandibular condyle. Surrounding portion of normal tissue must also be excised to prevent local recurrence. Chondroma is radioresistant. Moreover, radiation is not preferred because of the potential of these tumours to undergo malignant transformation later on.