Answer of September 2022
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
An 8-year-old boy was referred from Student Health Service for left hearing loss. His teacher complained him of poor hearing in school for a year. There was all along no otorrhea nor otalgia. On otoscopic examination, the tympanic membrane was intact and there was no evidence of effusion noted. Pure tone audiometry suggested left-sided hearing loss at 50dB with an air-bone gap. The working diagnosis was left-sided conductive hearing loss. High Resolution Computed Tomography of Temporal Bone was therefore arranged for further investigation.
Axial and coronal images of the left temporal bone:

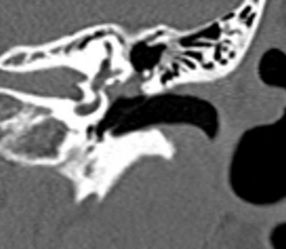
IMAGING FINDINGS:
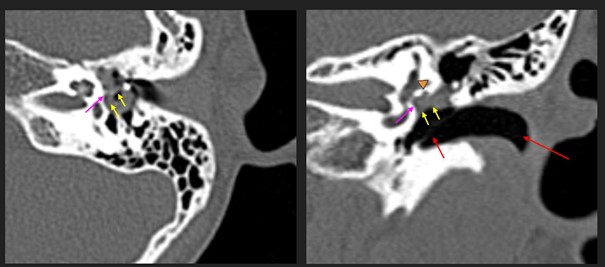
Axial and coronal images of the left temporal bone: There is soft tissue density in the epitymepanic space of the middle ear epicentered medial to the ossicular chains encasing the oval window (pink arrow). The long process of incus and the stapes appeared indistinct suggestive of erosions (yellow arrows). The tympanic segment facial nerve canal is being partially eroded (orange yellow head). The left tympanic membrane and external auditory canal are intact (red arrows). Features are consistent with congenital cholesteatoma.
DIAGNOSIS:
Congenital Cholesteatoma
DISCUSSION:
Cholesteatoma is a misnomer as it does not contain cholesterol and it is not a tumor. It is identical to epidermoid cysts, differing only in name and location. It is commonly described as “skin in the wrong place”.
Cholesteatoma are broadly classified as congenital form and the commoner acquired form. They are indistinguishable with histology and imaging. In fact, only the location of the lesion, the clinical history of the patient, and the otologic status of the tympanic membrane may give some hints for differentiating these two types of cholesteatomas. Congenital cholesteatoma can appear anywhere in the temporal bone. On the other hand, acquired cholesteatoma mainly occurs in middle ear. Second, patients with congenital cholesteatoma are typically children that are asymptomatic. On physical examination the tympanic membrane is typically intact. On the contrary, patients with acquired cholesteatoma are typically adults with recurrent ear disease e.g. otorrhea and otalgia. The tympanic membrane is typically perforated on examination.
Congenital cholesteatoma is first described in 1953 by House et al. Up to 1980, only 84 cases were reported in the literature. It is due to the inclusion of squamous epithelium within the temporal bone during development. It can occur anywhere in the temporal bone e.g. middle ear, mastoid, petrous apex, squamous part of the temporal bone, within the tympanic membrane, or in the external auditory canal. Levenson’s criteria for the diagnosis of congenital cholesteatoma consists of (1) white mass medial to a normal tympanic membrane, (2) no prior history of otorrhea, (3) no prior history of tympanic membrane perforation and (4) no prior history of any otoscopic procedure.
High Resolution Computed Tomography (HRCT) has the advantage of providing excellent spatial resolution for delineating the extent of this condition, together with the complications. Besides, it carries a high sensitivity of detecting this disease i.e. a high negative predictive value. Soft tissue density is typically observed medial to ossicular chain and fills oval window. It most commonly involves the anterior superior quadrant of the middle ear. Middle ear ossicular erosions can be observed in this disease. Magnetic resonance imaging is typically reserved for post-operative imaging. It is important to remember that cholesteatoma typically does not show enhancement on contrast enhanced imaging, while restricted diffusion is typically being observed. Non echo-planar imaging diffusion weighted imaging (non EPI-DWI) is helpful in the post-operative setting to detect residual or recurrent disease.
In our patient, endoscopic assisted atticotomy of left ear was performed and confirmed cholesteatoma over left oral window. The tympanic part of facial nerve appeared dishesicent intra-operatively. Erosions of long process of incus, stapes and stapedial tendon were seen. Operative biopsy findings were consistent with cholesteatoma.