Answer of August 2022
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 49 year old female complained of repeated episodes of vomiting and diarrhea for one year. Preliminary imaging in the private sector showed multiple intra abdominal lesions (images unavailable). Follow-up images are shown.
Triphasic CT:






IMAGING FINDINGS
Triphasic CT scan shows multiple bilobar hepatic hypodense lesions with hypoenhancement on portovenous phases. Of the lesions, several demonstrate avid arterial-enhancement with washout on portal venous/delayed phases, suggestive of hypervascular hepatic lesions.
A mesenteric mass measuring approximately 5.5 cm in diameter with internal calcifications and spiculated margins is noted. No clear fat plane is seen between the mass and the ileal loops. Diagnosis: Small bowel carcinoid with hypervascular hepatic metastases.
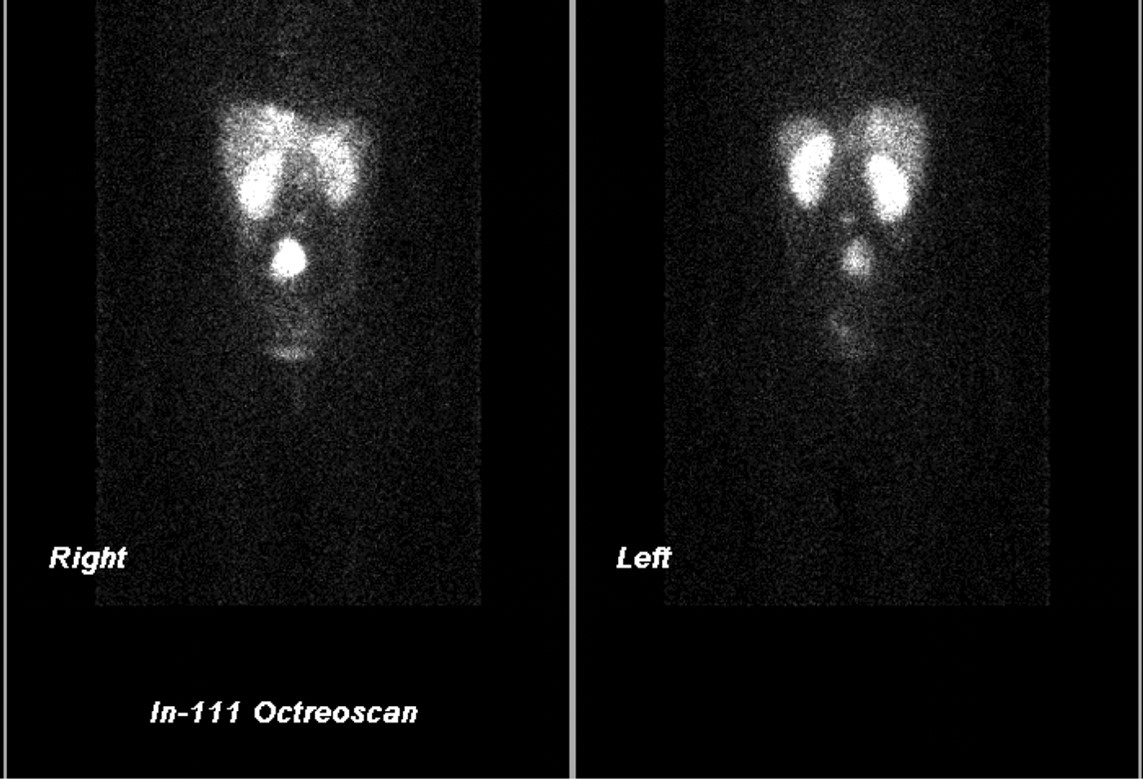
Correlation with In-111 Octreoscan for this patient: A sizeable mass with uptake is noted in the mid abdominal region corresponding to the CT-detected mesenteric mass. Multiple hepatic lesions with uptake are also noted. A L3 vertebral body focus with uptake is also suspicious of bone involvement.
The patient was found to have elevated serum chromogranin A (cGA), and 24-hr urine 5-hydroxyindoleacetic acid (5-HIAA), confirming the diagnosis of carcinoid tumor with metastases and carcinoid syndrome.
DISCUSSION
Carcinoid tumors are a type of neuroendocrine tumor arising from amine precursor uptake and decarboxylation (APUD) cells. Typical radiologic findings include enhancing lesion in the gastrointestinal tract or lungs, with rarer cases such as hepatic, thymic, and ovarian primaries also reported. The small bowel is the most commonly involved part of the gastrointestinal tract (40%), though carcinoid tumors can be found throughout the entire alimentary canal.
Carcinoid syndrome describes a clinical picture of episodic diarrhea, facial flushing, tachycardia, tricuspid valvopathy with right heart failure, and bronchospasm, postulated to be due to the vasoactive amines and peptides secreted by the carcinoid tumor (including serotonin, histamine, tachykinins, kallikrein, and prostaglandins). The vasoactive amines are metabolized and inactivated by the liver in the case of the common carcinoid involving the gastrointestinal tract. However, in cases of metastatic lesions, ovarian or lung carcinoids, the vasoactive substances secreted by the tumor are postulated to be able to bypass first pass hepatic metabolism to cause systemic effects. Thus carcinoid syndrome is observed in these minority circumstances.
When metastatic, carcinoid tumors often present with a hypervascular enhancement pattern. Radiologically, it is also important to consider the other possible causes of hypervascular metastases including pancreatic islet cell tumors, certain subtypes of thyroid carcinomas, choriocarcinoma, melanoma, clear cell renal cell carcinoma, metastatic hepatocellular carcinoma, leiomyosarcoma, and other neuroendocrine tumors, with their respective anatomic regions further scrutinized. Furthermore, primary hypervascular hepatic lesions should also be considered especially in localities with high hepatocellular carcinoma incidence.
Nuclear medicine studies may be helpful to aid in diagnosis of carcinoid, which can show uptake of Ga-68 DOTATATE, In-111 octreotide/pentetreotide, and I-123 MIBG, the former regarded as more accurate and preferred where available, owing to the higher resolution of PET-CT versus SPECT as well as its higher affinity for somatostatin receptor 2. Meta analyses of Ga-68 DOTATATE scan have also shown significant improvement for demonstrating disease extent of GI neuroendocrine tumors over In-111 octreoscan, with management-altering differences in up to 83% of patients in some series.
Where the radiologist is concerned with the management of metastatic carcinoid tumors, transarterial chemoembolization (TACE) or transarterial radioembolization (TARE) with Y90 have recently gained increasing recognition for the management hepatic metastases of carcinoid with conflicting evidence. Some studies have shown Y90 TARE to have a survival benefit. Repeat TACE for disease control has also been shown to result in biochemical responses, though due to an increase in morbidity, its lack of clear disease-free progression and survival benefit, leaves much for debate and further study.
For the patient mentioned in this report, 6-year follow up after 10 cycles of repeat TACE (cisplatin) with octreotide therapy showed minimal disease progression.