Answer of February 2022
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
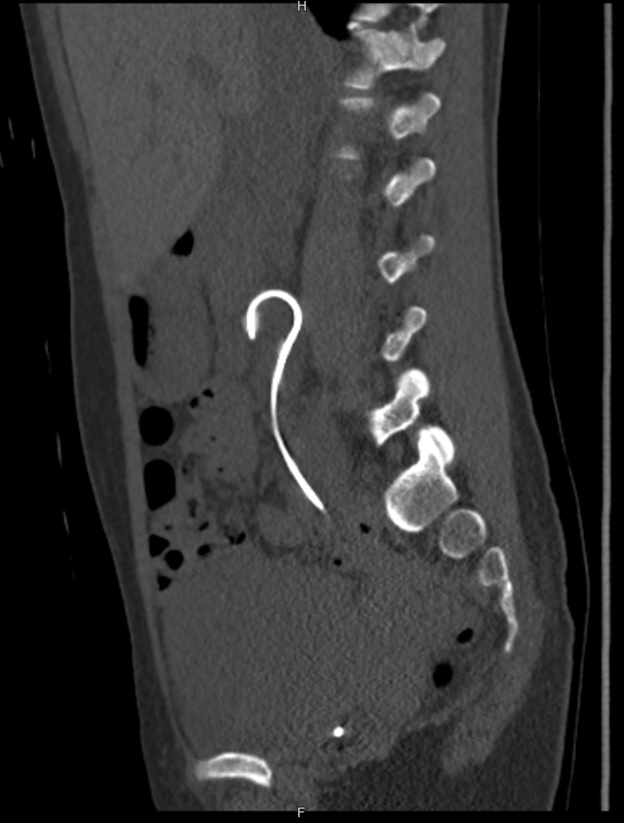
A 40-year-old lady presented as urosepsis during her pregnancy. USG found right hydronephrosis and ureteric stent was inserted by the urologist. A plain CT urogram was performed to evaluate the cause of her hydronephrosis after the delivery of the baby.




IMAGING FINDING
A layer of crystal deposition is seen at the renal and bladder ends of the stent, partially blocking the side holes. The ureteric stent is in-situ and remains intact.
DIAGNOSIS
Stent encrustation
DISCUSSION
Encrustation of ureteric stent is one of the complications of
ureteric stent placement. All stents are
not inert within the urinary tract. Therefore, deposition of urine constituents
can happen on any stents with time. It preferentially happens at renal or
bladder ends of the stent. It is postulated that the peristaltic “wiping”
makes the crystal deposition less likely occur along the ureteral portion of the
stent.
Risk factors for encrustations include prolonged indwelling stent duration, particularly more than 12 weeks, pregnancy, lithogenic urine, pregnancy and recurrent urinary tract infection. It can be prevented by high fluid intake to dilute the urine, aggressively treating the urinary tract infection, and regular prophylactic exchange of ureteral stents.
Mild stent encrustation would not affect the removal of the stent, and probably can be treated with extracorporeal shock wave lithotripsy (ESWL). However, serious encrustation can result in urinary tract injury or fracture of the stent if blind forceful stent removal is attempted. In that case, combinations of ESWL, percutaneous lithotomy, cystoscopic lithopaxy and open surgery may be needed.