Answer of December 2021
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 78-year-old lady with incidental finding of left neck mass on imaging.
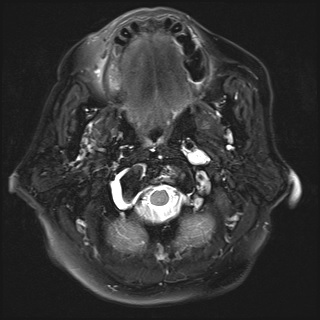
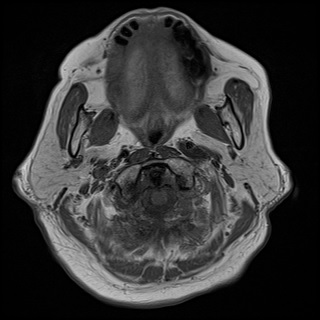
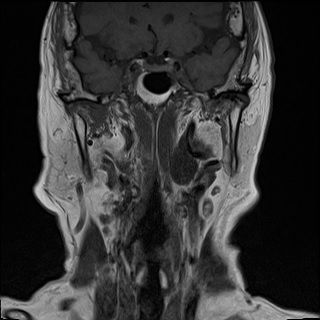
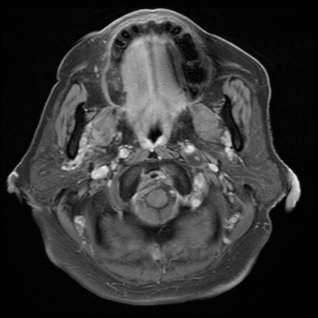
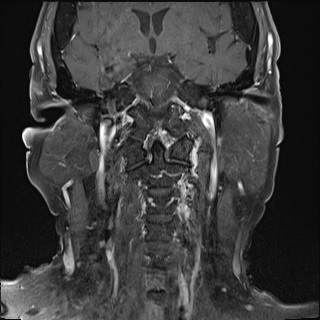
MRI neck (T2 weighted fat supressed, T1 weighted, T1 weighted fat supressed post gadolinium images):
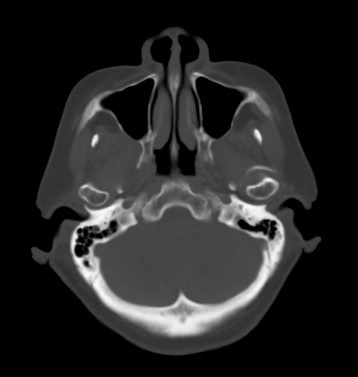
CT neck in bone window

IMAGING FINDINGS
MRI : A well circumscribed dumbbell shaped mass is seen at left jugular foramen with extension into left suprahyoid carotid space. The left internal carotid artery is encased with preserved flow void signal. The mass shows low signal on T1 weighted images and high signal on T2 weighted images with heterogenous enhancement. Non enhancing T2 weighted hyperintense area is suggestive of cystic component. There is no flow void signal on T2 weighted images nor “salt-and-pepper” appearance on T1 weighted images”. No dural tail sign is evident.
CT in bone window: The left jugular foramen is mildly enlarged with smooth bony margin. No bony destruction or hyperostosis is evident.
DIAGNOSIS:
Jugular foramen schwannoma
DISCUSSION:
Tumours involving the jugular foramen can be divided into primary or secondary tumours according to the anatomical origins. The most common primary tumours include glomus jugulare tumours (paraganglioma), schwannoma and meningioma, in descending order of frequency. Secondary tumours, which are far less common, are arise from other sites of skull base and secondarily involve jugular foramen. The main differentiating findings are major involvement of petrous bone and minor involvement of parapharyngeal space when compared with the primary lesions. Examples include skull base metastasis, chodroma, chondrosacroma.
Computed tomography (CT) and Magnetic resonance imaging (MRI) are helpful for characterisation and delineation of the extent and epicentre of the tumour. Schwannomas in jugular foramen can be originated from the ninth, tenth or eleventh cranial nerves, most commonly from the ninth cranial nerve. CT is particularly useful for analysis of bony margin of jugular foramen and bony changes in adjacent skull base and temporal bone as well as mineralisation of the tumour. In schwannomas, the jugular foramen is enlarged with smooth and well-defined bony margin. Hyperostosis around jugular foramen can occur in meningioma. Permeative bony destruction of the jugular foramen and demineralisation of the surrounding skull base or temporal bone are commonly seen in glomus jugular tumour. On MRI, it demonstrates a T2 weighted high signal and T1 weighted low signal with gadolinium enhancement. Approximately 24% of these lesions are primarily cystic or associated with cystic degeneration. There is no dural tail sign which is typically seen in meningioma. It is usually solid and circumscribed lesions. Paraganglioma is a hypervascular tumour, which demonstrates “Salt-and-pepper” appearance in T1 weighted image, flow voids signal in T2 weighted images with strong gadolinium enhancement. It is not well encapsulated and tend to infiltrate into different tissue planes. On angiogram, both meningioma and schwannoma demonstrate mild to moderate vascularity, while hypervascularity is demonstrated in paraganglioma. Peripheral primitive neuroectodermal tumour is another differential diagnosis. CT bone windows shows an enlarged jugular foramen with irregular contours, which allows differentiate from schwannoma and paraganglioma. MRI often shows irregular shaped mass with isointense on T1-weighted sequences and mild hyperintense on T2-weighted sequences.
There a staging system described by Samii et al based of the anatomic involvement of the tumor:
Type A: primarily intracranial with minimal
enlargement of jugular foramen.
Type B: Primarily in jugular foramen extending to surrounding bone.
Type C: primarily extracranial with extension into jugular foramen.
Type D: “dumbbell”-shaped appearance with both extra- and intracranial
components.
Enlargement of jugular foramen may not be seen in primary intracranial or
extracranial tumour (type A or C).