Answer of March 2021
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 13-year-old boy complains of left shoulder pain for 5 months and swelling for a few days. He is stable and afebrile at the time of examination.
 Left shoulder X-ray (AP) Left shoulder X-ray (AP) |
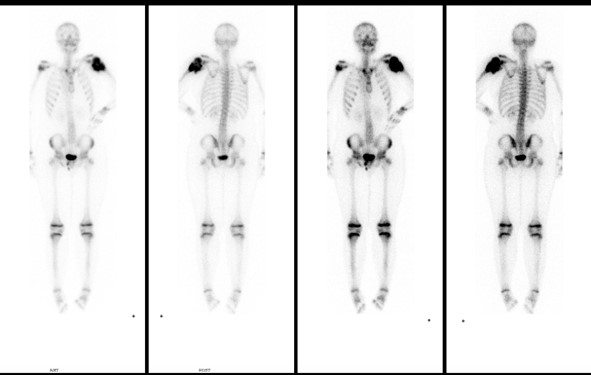 Whole body bone scintiscan Whole body bone scintiscan |
IMAGE FINDINGS:
Left shoulder X-ray showed left proximal humeral metaphysis mixed lytic and sclerotic changes with wide transition zone. Epiphysis of left proximal humerus is likely involved. Periosteal reaction with Codman’s triangle appearance and soft tissue mass with osteoid tumor matrix seen.
Whole body bone scan showed marked increased tracer uptake in left proximal humerus. No other evidence of bone metastasis.
DISCUSSION:
Osteosarcoma is the most common primary bone tumor in children and adolescents with male predominance and mainly produces osteoid matrix. They are classified as primary and secondary forms. Osteosarcoma is classified into different subtypes with distinct imaging features and prognosis. Conventional osteosarcoma (central osteosarcoma, high grade intramedullary osteosarcoma) is the most common subtype of osteosarcoma. They are commonly seen in the metaphyseal areas of long bones of the extremities with its occurrence in (descending order) distal femur, proximal tibia, humerus, etc. 50% is seen around the knee.iSecondary osteosarcoma occurs in elderly and is usually malignant transformation within benign process such as Paget disease, previous irradiation site. It presents as aggressive bone destruction in area of preexisting condition with large soft tissue mass. Secondary osteosarcoma has a much wider distribution and have much have a higher incidence in flat bones.
Pain is a common presenting symptom.
Plain X-ray is important first line imaging investigation. The characteristic radiological features are periosteal reaction with sun-burst, Codman’s triangle appearance, bone destruction with wide zone of transition, and soft tissues mass with tumor matrix ossification.
CT is predominantly utilized in assisting biopsy and staging. CT scan can delineate the bony anatomy more clearly and accurately.
MRI is used for local staging, accurately and precisely delineates (1) extent of the tumor, (2) involvement of joint, growth plate, neurovascular bundle (3) skip lesion ii (4) guide biopsy.
Tc99 MDP bone scan is the most commonly used investigation for detecting osseous metastasis. Lungs are also preferential site for osteosarcoma metastases, which are often ossified and some can show uptake in bone scan. CT thorax is commonly used for distal staging. Pulmonary metastasis from osteosarcoma can manifest as a spontaneous pneumothorax because they tend to be in subpleural location and may cavitate.
It is important that the patient should be immediately referred to the specialist center for sarcoma for early diagnosis and treatment. Biopsy should be performed after complete clinical history, examination and imaging. Orthopedic surgeon should be consulted to plan the biopsy track to reduce the chance of seeding.
Treatment is usually chemotherapy followed by wide surgical resection.
Predictors of poor outcome include metastasis at presentation, large size, pathological fracture and skip marrow lesions.
In the young patient with an aggressive lesion, the two main primary bone tumors to consider are Ewing’s and osteosarcoma. The two can be difficult to differentiate radiologically. Ewing’s sarcoma is the second most common malignant primary bone tumors of childhood after osteosarcoma. iii It tends to occur in younger patient, and more common in diaphysis. Ossification in soft tissue is commonly seen in osteosarcoma.