Answer of May 2020
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
Seven-year-old boy with swelling of left hand including the thumb and index finger since birth. Increased forearm swelling since one year ago.
  |
   |
  |
  |
  |
Imaging Findings:
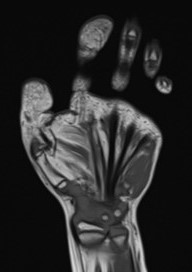
Radiographs:
- Clinodactyly of the left index finger.
- Bone expansion of thumb and index finger phalanges and associated soft-tissue expansion.
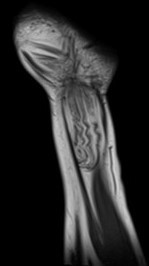
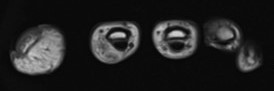
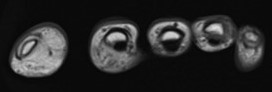
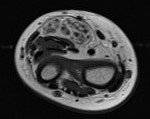
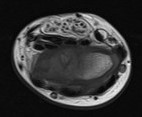
MRI:
- Fatty hypertrophy of the medial hand, involving the thumb, medial aspect of index finger with fatty infiltration of the thenar muscles.
- No dilated vasculature to suggest arteriovenous malformation nor venous malformation.
- Diffuse marked enlargement of the median nerve, which shows an increase of adipose tissue interspersed between the individual nerve bundles.
Diagnosis:
Focal gigantism (macrodystrophia lipomatosa).
Discussion:
Macrodystrophia lipomatosa (MDL) is a rare cause of congenital macrodactyly, characterised by progressive proliferation of all mesenchymal elements, with disproportionate increase in fibro-adipose tissue. It occurs most frequently in lower limbs along the distribution of the medial plantar nerve. MDL presents as localised gigantism of the hand or foot and comes to clinical attention for cosmetic reasons, mechanical problems secondary to degenerative joint disease, or development of neurovascular compression.
The disorder is congenital in origin, but not hereditary. It is characterised by excessive growth of fibro-fatty tissue with unusually large fatty lobules, apparently fixed by a mesh of dense fibrous tissue. Hypertrophy and tortuosity of the digital nerve, a striking feature in macrodactyly of the hand, is notably absent in cases affecting the foot.
Exact etiology of the disorder is not known. Probable mechanisms include: abnormal nerve supply, abnormal blood supply, or abnormal humoral mechanisms. The rate of accelerated growth varies among patients and also among affected digits. Progressive macrodactyly is more common than the static type. It can be present at birth along with syndactyly, digital deviation, thenar eminence hypertrophy, palmar and forearm hyperplasia. Association with small osseous protuberances resembling osteochondromas and lipomas in other parts of the body have also been reported. Its involvement is almost always unilateral as seen in our case. The lower limb is more frequently involved than upper limb, which is typically along a specific sclerotome, with the most common sites being second and third digits corresponding to the median nerve and medial plantar nerve in upper and lower limbs, respectively. Involvement of the fifth digit is a rare occurrence.
Plain films usually suffice and demonstrate splayed, lengthened and broadened phalanges with endosteal and periosteal bone deposition. The overlying soft tissues are markedly overgrown, especially in the volar and distal aspects. Within the soft tissues, focal lucent areas representing fat may be seen, which is characteristic.
MRI is helpful in distinguishing macrodystrophia lipomatosa from other causes of macrodactyly. It demonstrates accumulation of fat in the subcutaneous tissues without a discernable capsule. There might be fibrous strands seen within this accumulated fat with cortical thickening, osseous hypertrophy and bony outgrowths from the underlying bone. Neural thickening may also be visualized.
Although macrodystrophia lipomatosa is considered a progressive form of macrodactyly, growth halts at puberty. As such treatment is reserved for cosmesis and when the mechanical function is impaired.
Amputation is the ultimate therapeutic modality and it is indicated in most cases involving the large digits. Other surgical procedures performed in macrodactyly include stripping of the nerves from their branches or removal of a part of the nerve and end-to-end anastomosis to relieve pain.