Answer of February 2020
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 38 year old female with history of chronic alcoholism and substance abuse presents with coma. MRI was performed.
Discussion:
Wernicke's encephalopathy (WE) is an acute neurologic disorder resulting from thiamine (vitamin B1) deficiency.
Traditionally, the clinical diagnosis of WE rests on the classical triad consisting of ocular signs, altered consciousness, and ataxia, described by Wernicke in his original article.
However, subsequent studies have revealed that this triad occurs in only 16–38% of all patients with WE, which explains at least in part why WE is often clinically underdiagnosed. WE may also evolve into the chronic form of thiamine deficiency known as Korsakoff psychosis, characterized by memory loss and confabulation..
Many clinical conditions can impair the correct absorption of an adequate amount of thiamine, including chronic alcohol abuse, gastrointestinal surgery, prolonged vomiting, chemotherapy, systemic infectious and noninfectious diseases, and dietary unbalance. Alcoholism does not directly cause thiamine deficiency, although it may induce such deficiency because of its frequent association with malnourishment.
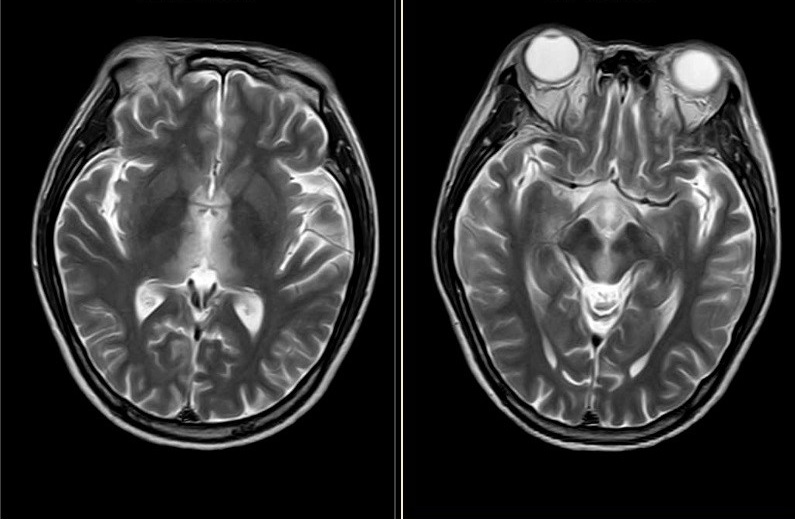
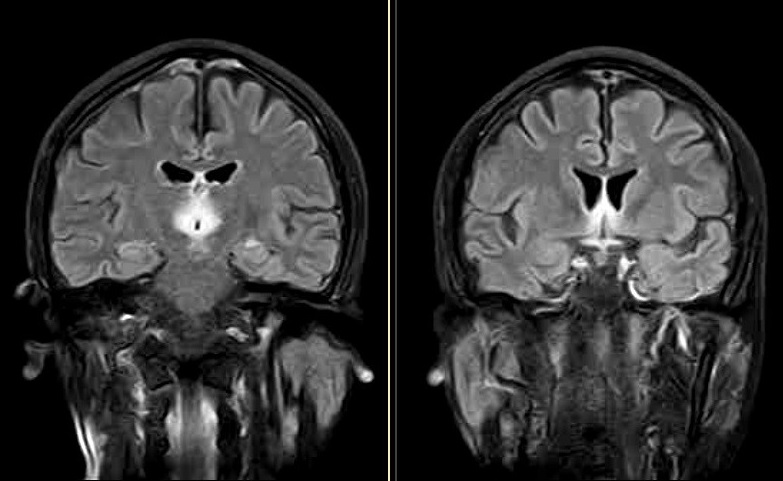
Reversible cytotoxic edema is considered the most distinctive lesion of WE, and it is easily shown on MR images. Typical findings are represented by symmetric alterations in the thalami, mamillary bodies, tectal plate, and periaqueductal area.
The anatomic regions most frequently involved by MRI in WE are the medial thalami and the periventricular regions of the third ventricle.
Treatment of acute WE is with intravenous thiamine infusion. The untreated mortality rate is up to 20%.