Answer of September 2019
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
This 51-year old gentleman presented with fever and abdominal distension and was noted to have a large abdominal mass on physical examination. CT of the abdomen and pelvis was performed.
|
|
|
|
|
|
|
|
|
|
|
|
 |
 |
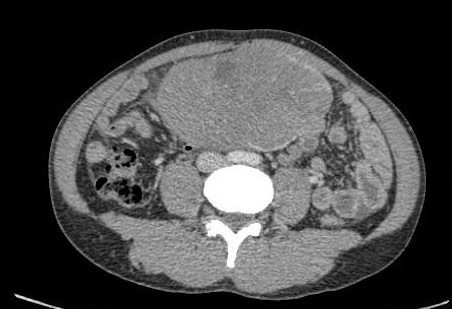

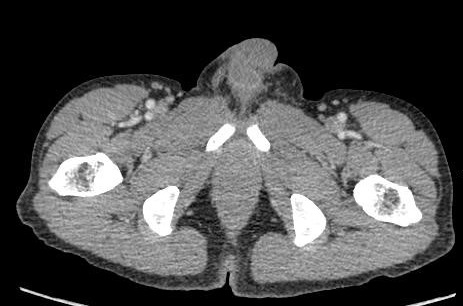


Imaging Findings:
A large lobulated solid mildly enhancing mass with intralesional vessels in the central lower abdomen, abutting upon the dome of the urinary and displacing adjacent small bowel loops, with peripheral claw of enhancing vessels supplying that are suggestive of left gonadal vessels. The left lower inguinal canal / upper scrotum is devoid of the spermatic cord (present normally on the right side). The scrotal sacs are not included in the scan. Prominent para-aortic lymph nodes up to 0.8cm present.
Diagnosis:
Undescended left testis with malignant degeneration
Discussion:
Undescended testis occurs in about 1-4.5% of newborns with a higher incidence in preterms (30-45%) (Acerini et al. 2009) (Ashley et al. 2010). The testes initially develop in the abdomen and begin to migrate into the inguinal canal at ~21 weeks after conception, reaching the scrotum by 30 weeks. Failure of descent into the scrotum results in cryptorchidism.
Cryptorchidism is a well-documented risk factor for testicular cancer, with probability of developing a testicular germ cell tumour being 1:2000, that is 32-fold increase compared to the general population. The risk for intra-abdominal testicle is five times higher than for inguinal cryptorchidism. (3). Orchiopexy is the preferred mode of management in cases of viable testes as it reduces the risk of testicular cancer if performed before puberty and allows increased surveillance for testicular masses by physical examination.
In men with untreated cryptorchidism, an undescended testis with secondary malignancy may be seen as an intra-abdominal mass on imaging. When approaching a large intra-abdominal mass, the supplying or draining vessels may be of important diagnostic value as they may provide diagnostic clues to the organ of origin of the tumour, as in our case. Large intra-abdominal testicular malignancy may mimic mesenteric or bowel tumours. An empty ipsilateral scrotal sac, if included in CT, is also another diagnostic clue for cryptorchidism.