Answer of July 2019
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 57 year-old gentlemen with good past health presented with rapidly deteriorating memory loss and personality change in recent 3 months. Physical exam revealed no focal neurological deficits. Thyroid function test, B12 and folate levels were normal, screening test for syphilis was negative. Initial CT Brain showed no focal intracranial abnormality. MRI Brain was performed.
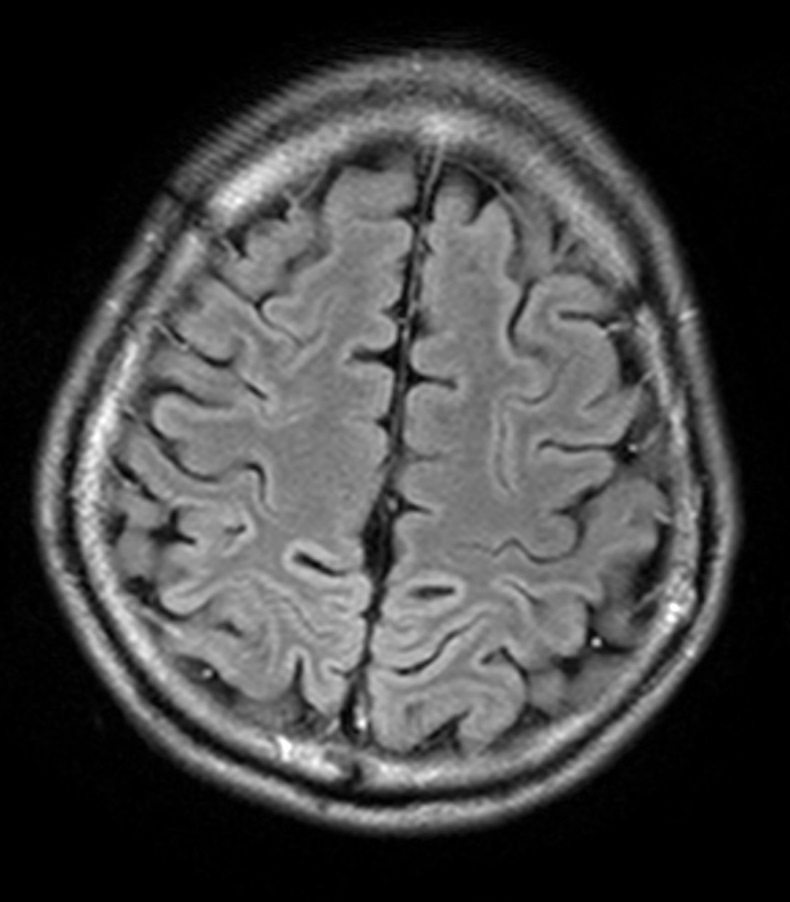
Image 1 of 6
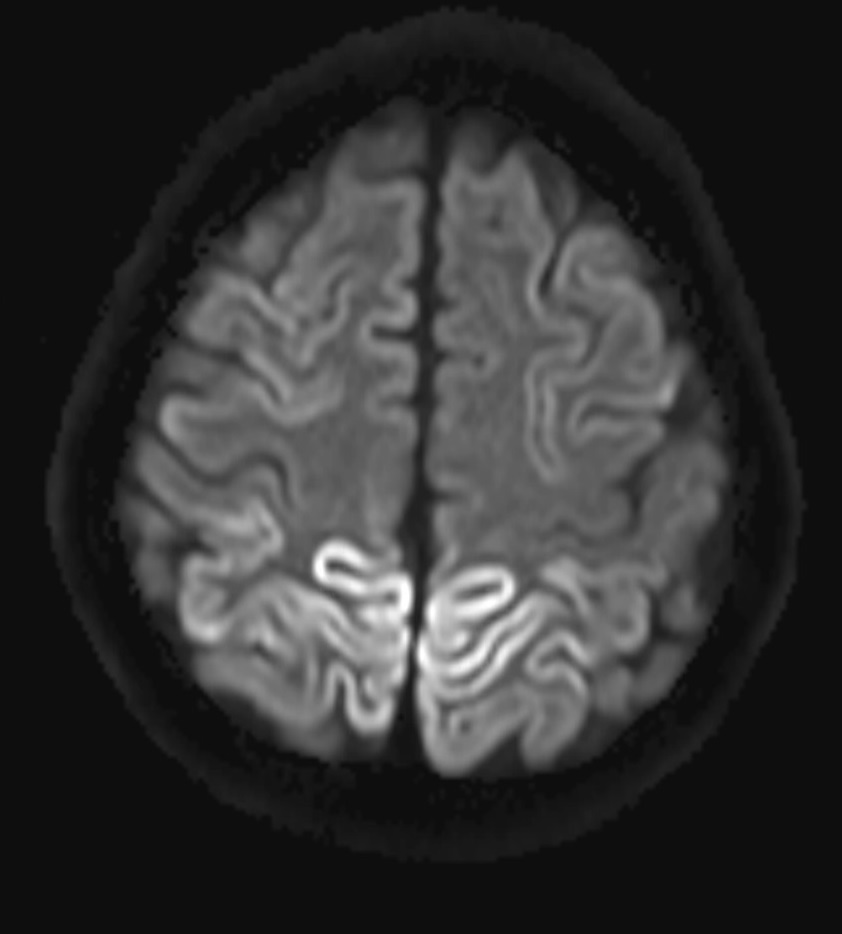
Image 2 of 6
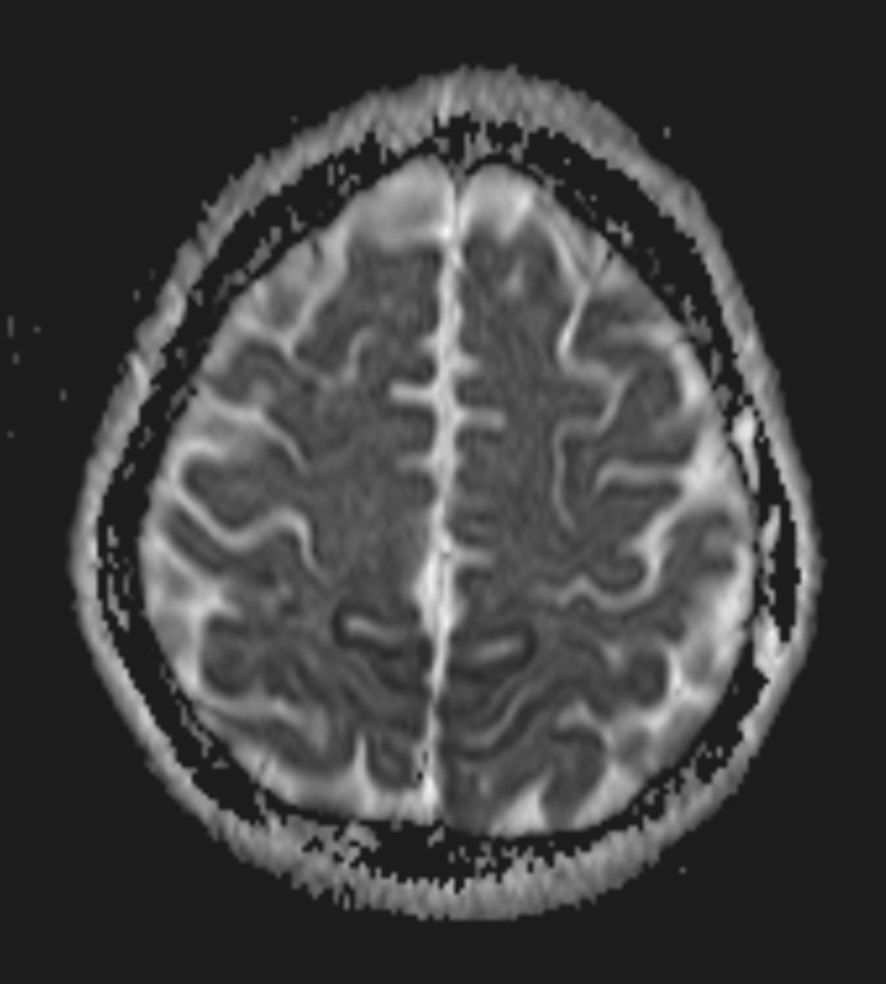
Image 3 of 6
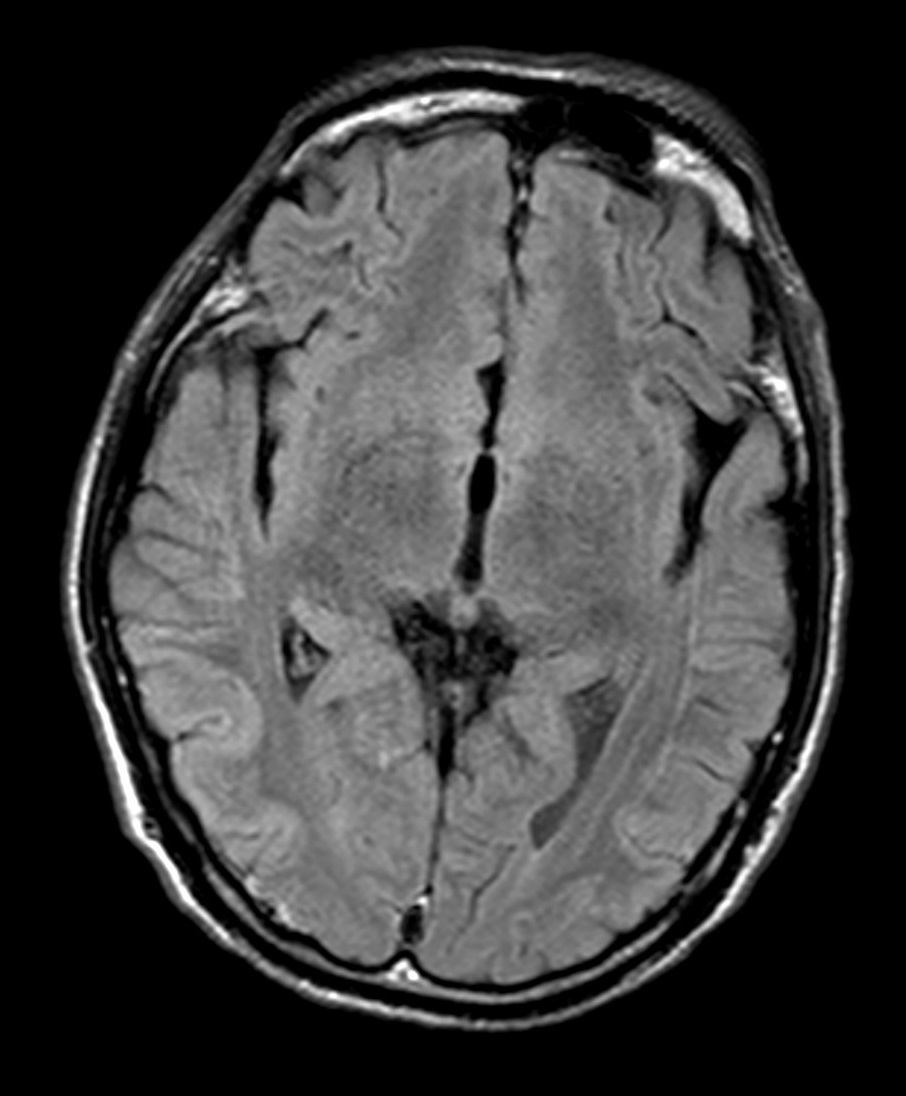
Image 4 of 6
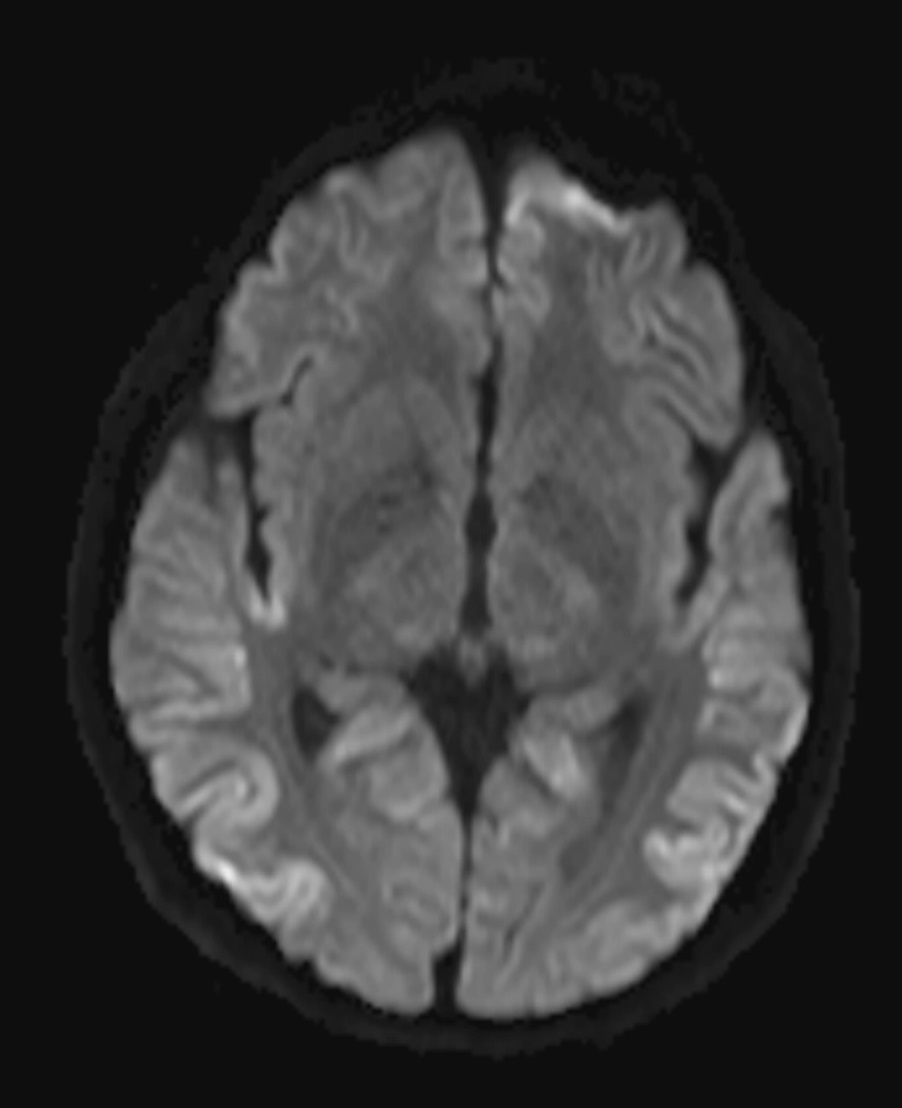
Image 5 of 6
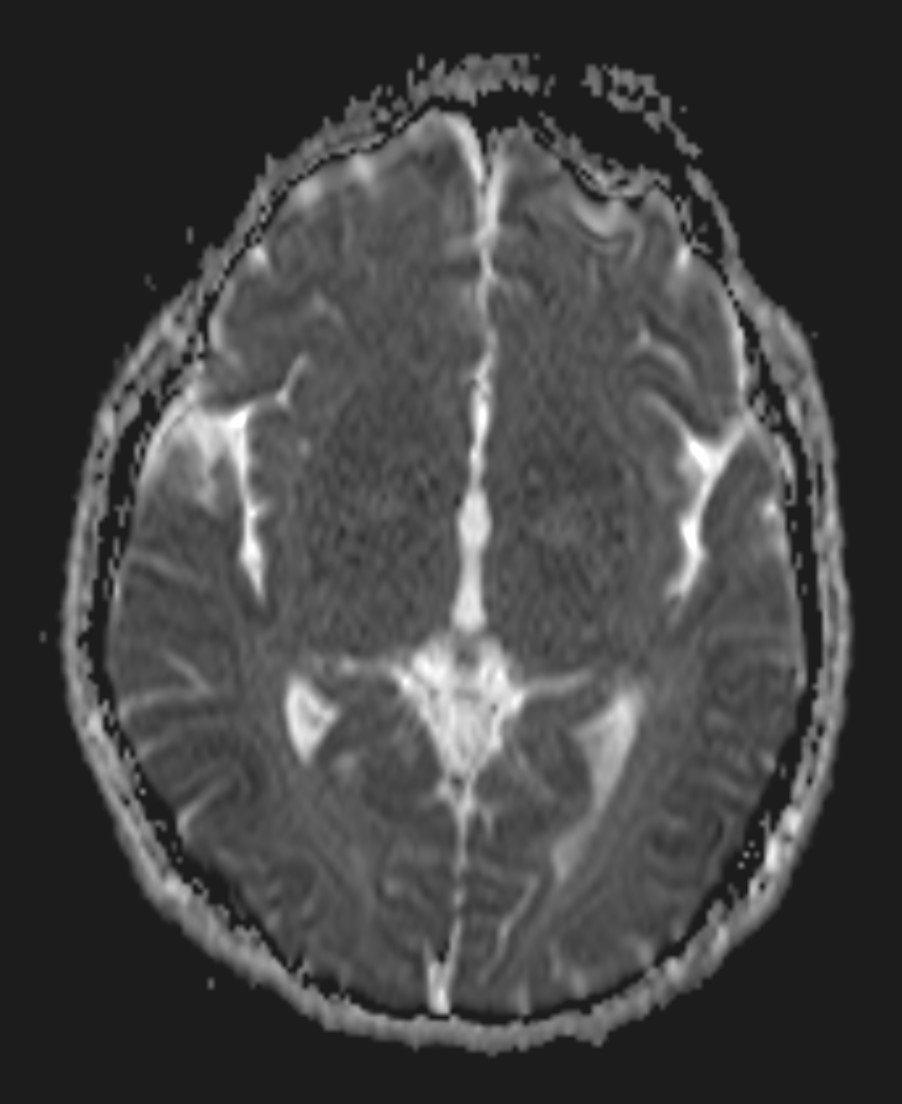
Image 6 of 6
Imaging Findings:
- Cerebral cortex: symmetric T2W FLAIR and DWI hyperintensities along cortical gyri (cortical ribbon sign) at bilateral occipito-parietal lobes, more conspicuous on DWI. Restricted diffusion is seen. Underlying white matters show no abnormal signal intensities.
- Basal ganglia: no abnormal signal intensity or restricted diffusion detected.
Diagnosis:
Sporadic Creutzfeldt-Jakob disease (sCJD).
Discussion:
Creutzfeldt-Jakob disease (CJD) is a rare, rapidly progressing, fatal neurodegenerative disease, characterized by spongiform encephalopathy. It is caused by infectious proteinaceous particles without nucleic acid, known as prions.
It can be divided into 4 subtypes according to the etiology, including: sporadic (sCJD), variant (vCJD), familial (fCJD) and iatrogenic (iCJD). sCJD is the most common subtype, accounting for 85-95% of the cases. It is caused by spontaneous conversion of PrPc to PrPsc.
CJD characteristically manifests as rapid neurological deterioration, including dementia, myoclonic jerks, pyramidal and extrapyramidal tracts dysfunctions, cerebellar signs, etc.
Gold standard test for sCJD is still brain biopsy, but it is invasive and is reserved for patients with suspected sCJD with other tests being non-diagnostic. Other investigations available include:
1. MRI Brain: imaging abnormalities of sCJD could be seen at cerebral cortex, basal ganglia and cerebellum:
- Cerebral cortex: symmetric or asymmetric DWI and FLAIR hyperintensity along cortical gyri (cortical ribbon sign), with restricted diffusion. Peri-rolandic areas are usually spared.
- Basal ganglia: symmetric or asymmetric DWI and FLAIR hyperintensity, particularly involving caudate and putamen. Signal abnormality progresses with disease.
- Cerebellum: cerebellar atrophy.
2. EEG: characteristic 1Hz biphasic or triphasic periodic sharp wave complexes.
3. Lumbar puncture and CSF analysis:
- 14-3-3 protein: sensitivity of 92% and specificity of 80%;
- Real time quaking-induced conversion (RT-QuIC) assays: sensitivity of 92% and specificity of 100%.
No curative treatment is available. Patients suffering from CJD have poor prognosis with mean survival of about 7 months.