Answer of March 2019
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 35 year old man presented with chronic right anterior knee pain for a few years especially on walking stairs.
MRI of right knee images.
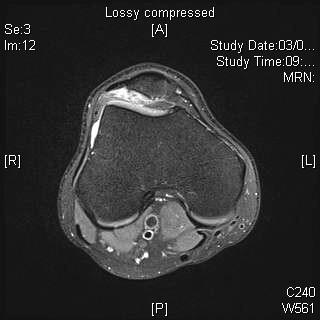
Axial T2 FS
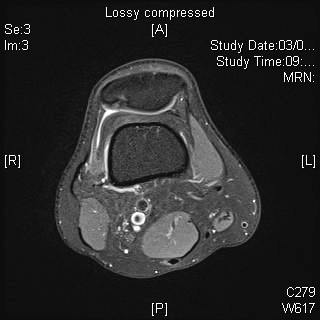
Axial T2 FS
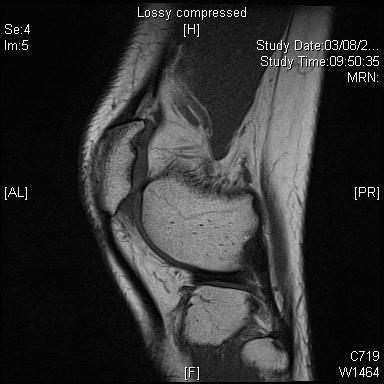
Sagittal T1
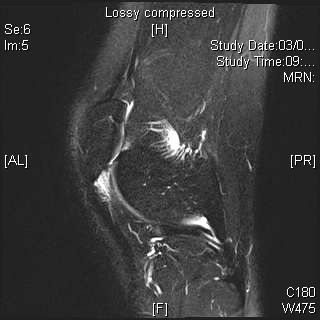
Sagittal T2 FS
Imaging Findings:
Increased signal at lateral Hoffa's fat pad interposed between lateral aspect of patellar tendon and the lateral femoral condyle.
No patella alta.
Focal small abnormal signal at lateral facet right patella cartilage associated with subchondral marrow signal, suggestive of chondromalacia.
Diagnosis:
Hoffa fat pad impingement syndrome
Discussion:
Hoffa fat pad impingement syndrome, also known as patellar tendon-lateral femoral condyle friction syndrome, is a common cause of chronic anterior knee pain and more prevalent among active females. It is a clinical syndrome characterised by anterior knee pain exacerbated by knee hyperextension. Clinical examination usually reveal focal tenderness in lower pole of patella.
Hoffa fat pad is one of the three peripatellar fat pads and it serves as a intracapsular extrasynovial protective cushion to reduce friction between the trochlear articular surface and proximal tibia. Patellar and trochlear dysplastic morphology increase the chance of patellar maltracking or lateralization during knee extension. The superolateral aspect of Hoffa fat pad (infrapatellar) may then be impinged. With repetitive microtrauma, inflammation leads to pain. Patella alta (Insall Salvati ratio >1.3 or modified Insall Salvati ratio >2), abnormal TT-TG ratio (>10mm) and increased patella tilt (>13.5 degrees) are significant predisposing risk factors.
MRI imaging findings typically show a focal area of high T2 signal in keeping with edema at superolateral aspect of Hoffa fat pad. Sometimes a cystic lesion may be found between the lateral femoral condyle and lateral retinaculum. Less common finding would be focal patellar tendinopathy manifested as thickening and increased signal change. There may also be cartilage loss and osteoarthritis in patellofemoral compartment.
Treatment is by conservative management with analgesics and NSAIDS together with physiotherapy.