Answer of August 2018
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
This 10 year old girl presented with right ear conduction hearing loss. She studies at a mainstream school, and her body height is in 10-25% range of the age-matched population.
She was noted to have dysmorphism with hypertelorism and bifid uvula, and her father shares the same features.
  |
|
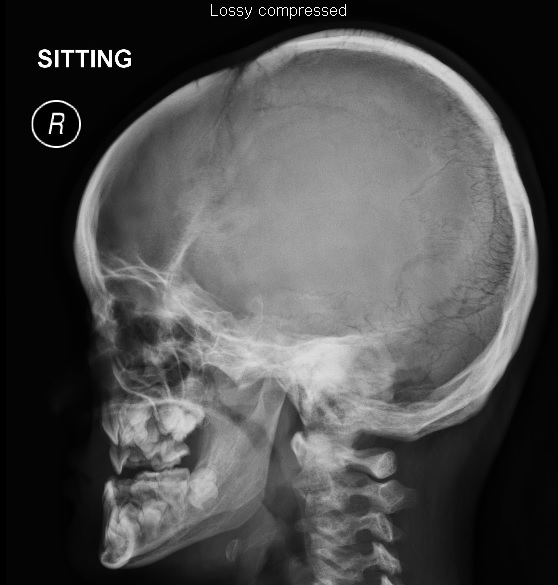
Image
1 : Skull radiographs, frontal and lateral views |
 |
|
Image
2: Pelvic radiograph (frontal view) |
 |
|
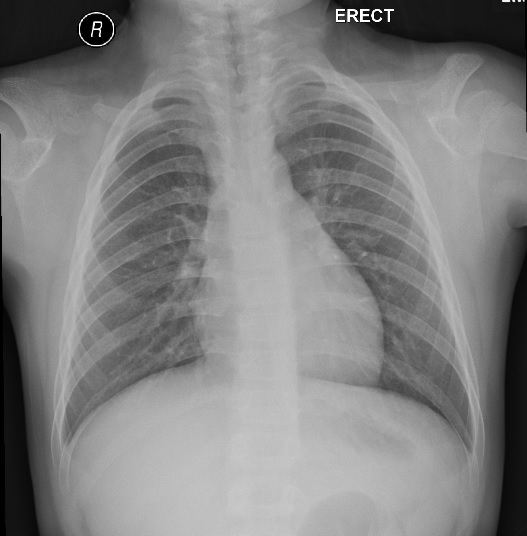
Image
3: Chest radiograph (frontal view) |
 |
|
Image
4: Frontal left hand radiograph. |
Imaging Findings:
Classic findings of cleidocranial dysplasia are shown:
Skull: persistent anterior fontanelle, wormian bones, frontal bossing, midface hypoplasia.
Chest: absent clavicles.
Pelvis: pseudo-widening of the symphysis pubis.
Hand: long second metacarpal, short second and fifth middle phalanges, tapered distal phalanges.
Discussion:
Cleidocranial dysplasia (CCD) is a rare autosomal dominant condition that also sometimes occurs through sporadic mutations of the RUNX2 gene at chromosome 6p21, which encodes a protein that affects osteoblastic differentiation and bone formation. CCD is characterized by abnormalities involving bones derived from intramembranous and endochondral ossification, especially the skull and clavicles.
The condition has no gender or ethnic predilection, and diagnosis is based on clinical and genetic findings.
Some patients can be identified in infancy on the grounds of short body length and a soft skull. Other patients may present in late childhood or adolescence with short stature, dental problems or hearing problems.
Facial characteristics include hypertelorism, midface depression (hypoplasia), supernumerary teeth with a predisposition to dental caries, high arched palate and bifid uvula.
Patients are susceptible to dental caries, impacted teeth, and dentigerous cysts.
Patients are also vulnerable to hearing problems related to Eustachian tube dysfunction and narrowed external auditory canals.
Patients can have hypermobility of the shoulders as a result of partial or total absence clavicles.
Most patients have normal intelligence.
Radiographic findings include the following:
1. Skull: delayed closure of sutures and fontanelles (which can remain patent into adulthood), frontal bossing, multiple wormian bones supernumerary teeth, midface hypoplasia, underdeveloped paranasal sinuses. Non-union of mandibular symphysis may be present.
2. Clavicles: reduced to single or double fragments, with the middle or lateral part being deficient. Complete aplasia (as in this patient) may be present.
3. Pelvis: Patients can have absent or delayed ossification of pubic bones, producing apparent widening of the symphysis pubis.
4. Appendicular skeleton:
i. Lower Limbs: Coxa vara or valga, Shortened or absent fibulae. Congenital pseudoarthrosis of the femur can occur.
ii. Upper Limbs: Patients can have long second and fifth metacarpals, short second and fifth middle phalanges, and tapered distal phalanges.
For the other differential diagnoses given in the question, these do not present with persistent anterior fontanelles or absent clavicles.