Answer of July 2018
For completion of the online quiz, please visit the HKAM iCMECPD website: http://www.icmecpd.hk/
Clinical History:
A 31-year-old gentleman presented with right hip pain of insidious onset for 3 months. The patient enjoyed good past health and there was no history of trauma. X-ray, CT and MRI of the pelvis were performed.
|
|
X-ray pelvis
|
|
|
X-ray right hip (Lateral oblique)
|
|
|
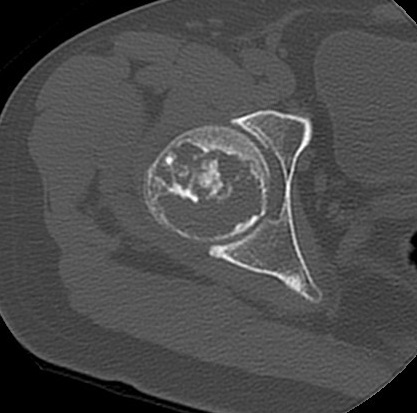
Axial CT right hip
|
|
|
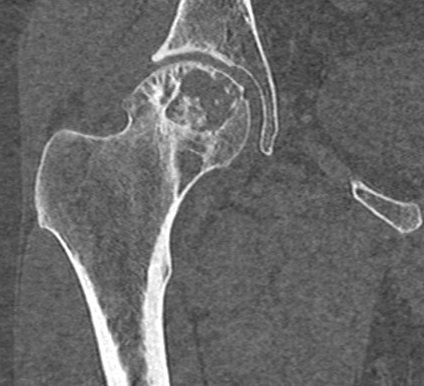
Coronal CT Right Hip
|
|
|
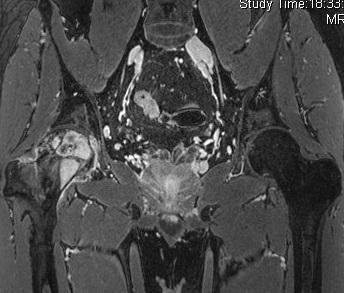
Coronal MR images of both hips (T1W, T2W-FS, T1W post-contrast)
|




Diagnosis:
Clear cell chondrosarcoma of right proximal femur.
Imaging Findings:
X-ray
- Mildly expansile geographic osteolytic lesion with intralesional sclerosis at epiphyseal-metaphyseal region of proximal femur.
- Narrow zone of transition and absent periosteal reaction.
CT
- Intramedullary lytic lesion at proximal femur with intralesional chondroid matrix calcification, endosteal scalloping and thin sclerotic border.
MRI
- Lobular enhancing mass with heterogeneous intermediate T1W and high T2W signal intensities at right proximal femur.
- Intralesional T1W/T2W hypointense foci corresponding to areas of matrix calcifications.
- Mild perilesional marrow edema and reactive changes at adjacent soft tissues.
Discussion:
Clear cell chondrosarcoma (CCCS) is a low-grade malignancy accounting for 1-2% of all chondrosarcoma. Histologically it is characterized by large neoplastic cells with abundant clear vacuolated cytoplasm with lobulated growth pattern. It most commonly involves patients in their third or fourth decades, with male twice more likely affected than female. Recurrence is frequent if CCCS is treated with simple excision and curettage and therefore the treatment of choice is wide local resection.
Long bones are affected in up to 90% of cases of CCCS, most commonly the proximal femur, followed by proximal humerus and around the knee. Lesions in the proximal humerus may show more aggressive features. Radiologically, CCCS typically appears as a geographic osteolytic lesion in epiphyseal-metaphyseal region of long bone. The zone of transition is variable but thin sclerotic rim can be present. Mild bony expansion is seen in around 20% of cases and chondroid matrix calcifications can be identified in more than one third of long bone lesions. Periosteal new bone formation is usually absent.
On MRI, CCCS shows heterogeneous low/intermediate T1W and high T2W/STIR signal intensities. Multilocular appearance and intralesional cystic changes which appear as bright T2W foci with fluid-fluid levels can sometimes occur. Mineralization, osseous metaplasia or hemorrhage may result in heterogeneous signals on T1W and T2W images. Perilesional marrow edema is usually absent or mild. Surrounding soft tissue changes, if present, should prompt one to search for pathological fracture.
The list of differential diagnosis in this case includes giant cell tumor, chondroblastoma, avascular necrosis and geode/subchondral cyst. On MRI T2W images, giant cell tumor and chondroblastoma usually exhibit low to intermediate signal intensities, while avascular necrosis often shows ‘double line sign’. Prominent bone marrow edema, which is mild in this case, is often seen with chondroblastoma. The lack of degenerative changes (such as joint space narrowing and marginal osteophytosis) in right hip joint renders the diagnosis of geode/subchondral cyst unlikely.
Results of CT guided percutaneous bone biopsy were suggestive of chondrosarcoma. The patient finally underwent partial ostectomy of right proximal femur and right hemipelvis and right total hip replacement. Final pathology was compatible with clear cell chondrosarcoma.