| ||||||||||||




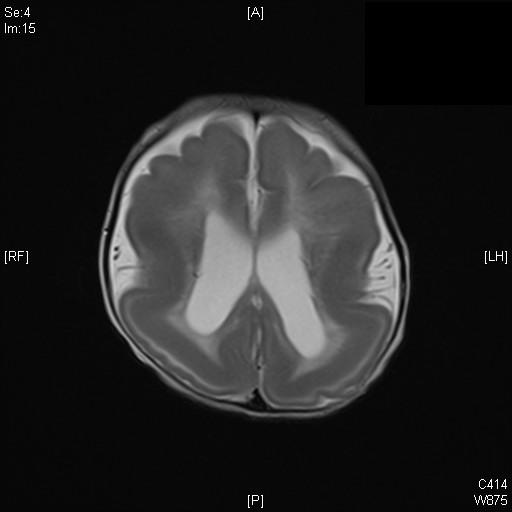

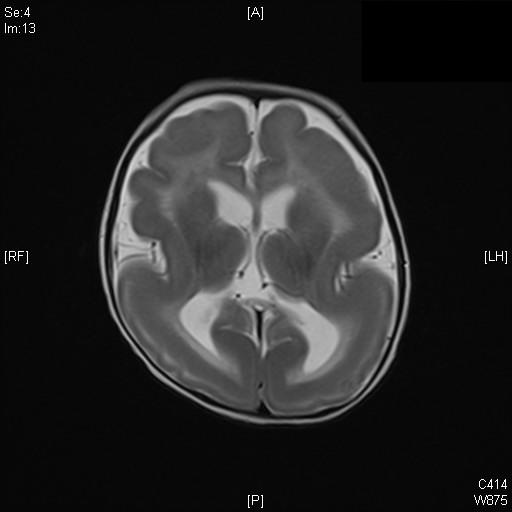
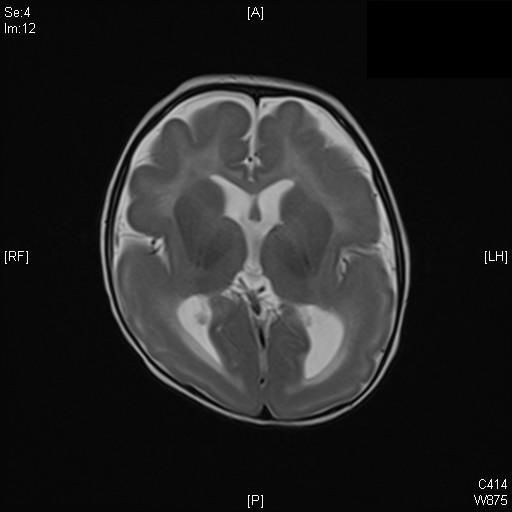
CLINICAL HISTORY: DIAGNOSIS: DISCUSSION: Features are compatible with type 1 lissencephaly with subcortical band heterotopia. Lissencephaly is a form of cortical formation disorder. The development of cerebral cortex can be divided in to 3stages: cell proliferation, cell migration and cortical organization. Cortical malformation can occur if any insults during these 3 phases of neuronal development. The cause of lissencephaly is not well identified yet. However, it is believed that genetic plays an important role in pathogenesis. Other proposed causes include viral infection or insufficient cerebral blood supply during early pregnancy. Lissencephaly can be divided in to two categories: Type I (classic) and Type II (cobblestone complex). MRI is one of the best imaging modality in characterization of the abnormality and to look for association. Type I lissencephaly usually has a smooth brain surface, or more commonly smooth brain surface with some gyral formation. These gives rise to abnormal brain outline resembling an hour glass or figure of 8 appearances on axial imaging. The cortex is markedly thickened and occasionally associated with subcortical band heterotopia. Unlike neuroal under-migration in Type I lissencehpaly, Type II lissencephaly is due to over-migration. As a result, it is characterized by a nodular brain surface. It is a heterogenous group of disorder and associated with ocular anomalies and congenital muscular disorderes. The three most common forms include: Walker-Warburg syndrome, Fukuyama congenital muscular dystrophy, and muscle-eye brain disease. Prognosis of lissencephaly varies depending on the type of malformation. Usually the child would be suffering from metal retardation, hypotonia, and seizure refractory to medication. Aspiration and respiratory diseases are the most common causes of morbidity and mortality.
|
||
PREVIOUS CASES |
||
HOME |
COMMENTS |
|