| ||||||
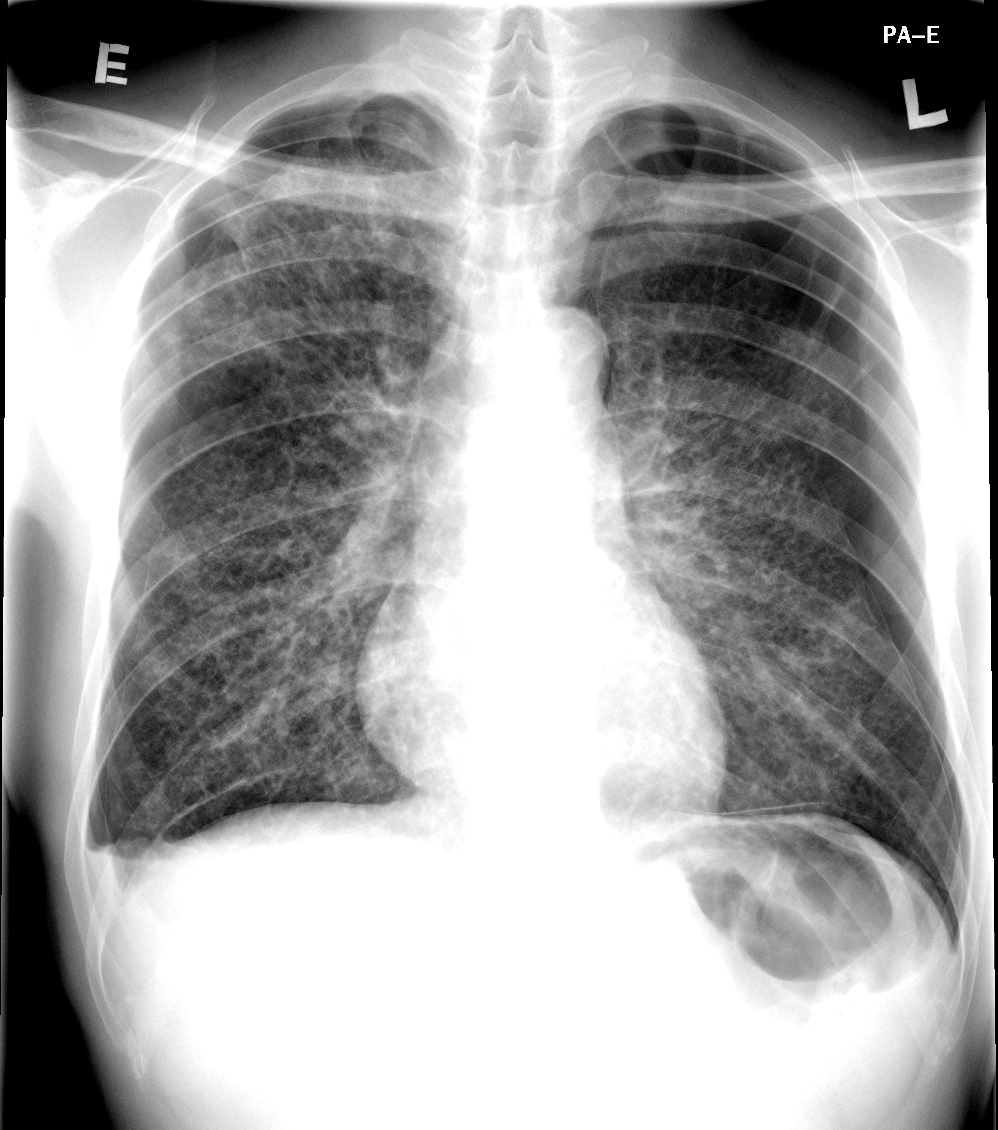

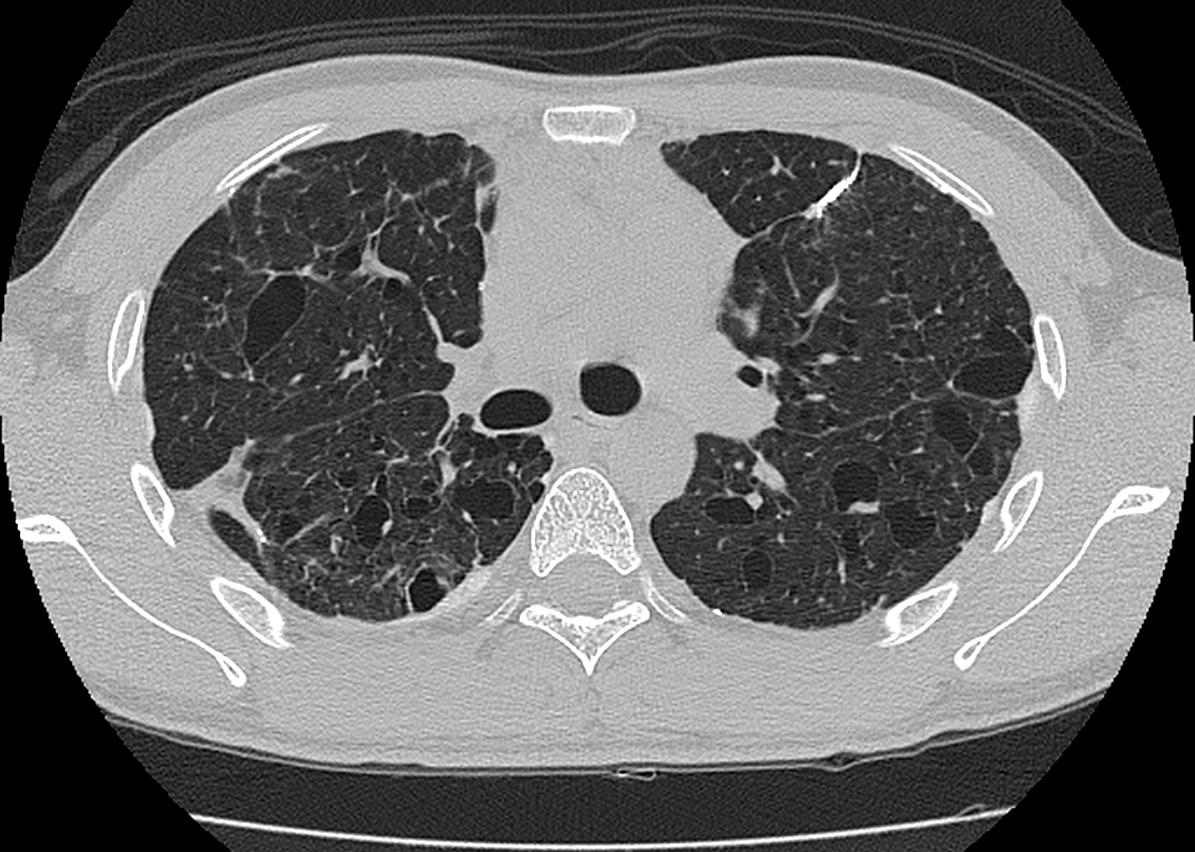

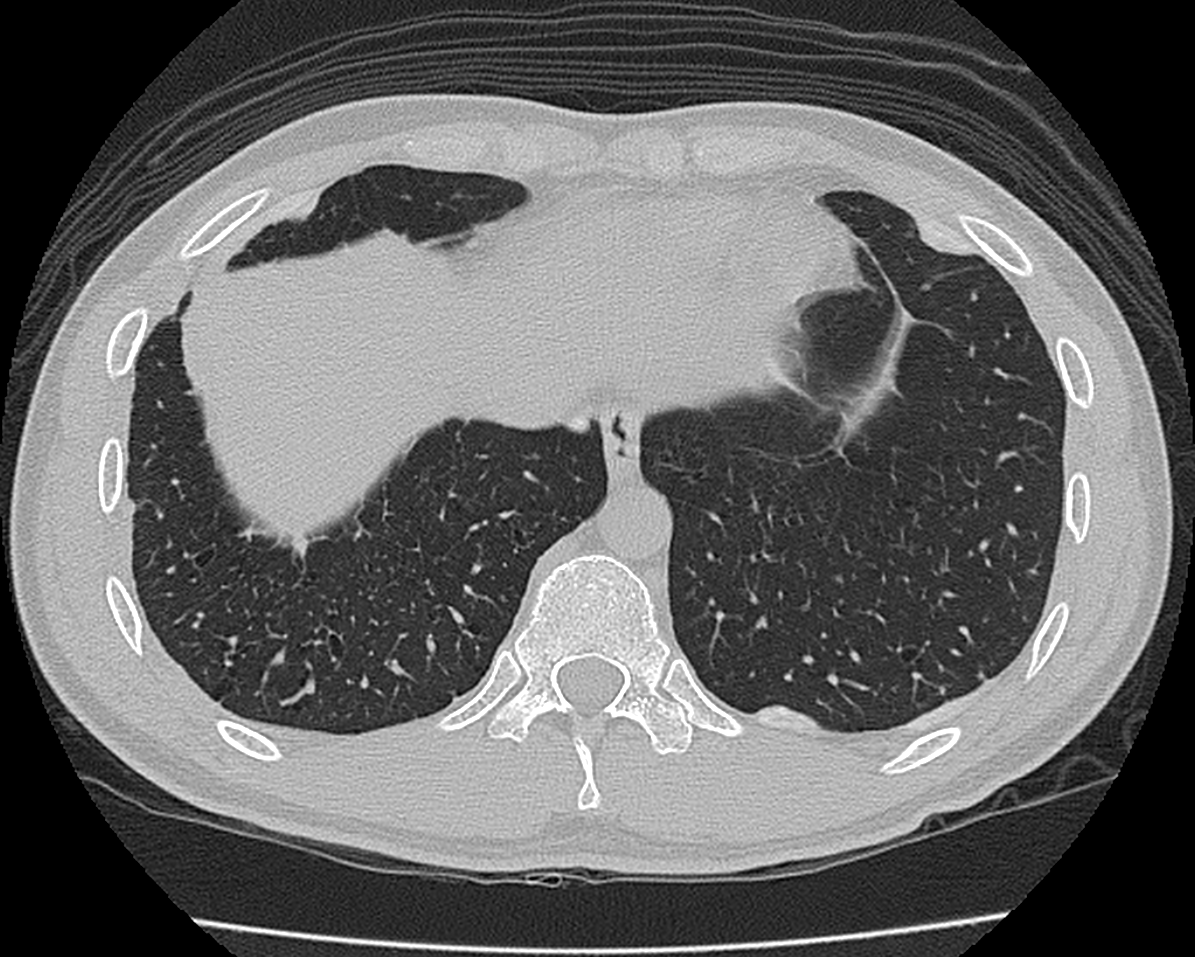
CLINICAL HISTORY: A 25 years old gentleman with unremarkable past health presented with acute onset of shortness of breath with chest pain. Chest X-ray on admission and subsequent high-resolution CT thorax taken a few months latter were available. DIAGNOSIS: DISCUSSION: Isolated pulmonary LCH occurs predominantly in young adults, with a peak frequency between 20 and 40 years ago. In the contrary, multifocal and systemic forms of LCH are usually seen in infants and children, and pulmonary involvement is not a prominent feature in these patients. A male predominance of the disease has been reported. Smoking is highly related to the development of pulmonary LCH but no direct correlation between the degree of cigarette consumption and disease severity has been demonstrated. Clinical presentations of pulmonary LCH include dry cough and dyspnea on exertion. Acute presentation of chest pain is more frequently a symptom of pneumothorax which can be seen in 10-20% of patients. Extrapulmonary manifestations of the disease can include symptoms related to pituitary (e.g. diabetes insipidus), bone or skin involvement. Not uncommonly, the disease presents as an incidental finding on a routine chest x-ray and it has been reported to represent up to 36% of patients. Physical examination is usually unremarkable except for patients complicated with pneumothorax or cor pulmonale, or presented with other extrapulmonary involvement. Radiographic features of pulmonary LCH vary depending on the stage of the disease. A proposed progression of imaging abnormalities starts with solid nodules which then become cavitary nodules, thick-walled cysts, thin-walled cysts and confluent cysts. On initial stage, multiple bilateral small lung nodules can be seen on chest radiographs. As these nodules undergo cystic degeneration, a cystic or reticular pattern hence predominates in the latter stage of the disease. The upper and middle zones are involved to a greater extent than the lung bases, which is related to the inhalation component of the disease. Lung volumes are usually normal or increased. Skeletal manifestation of the disease and complication of pulmonary involvement including pneumothorax or cor pulmonale are other features on chest radiographs. On high resolution CT thorax, there is typically presence of lung nodules together with cysts of variable wall thickness with upper zone predominance and sparing of the lung bases. A predominant nodular pattern can be seen in early stage where predominant thin-wall cysts can be seen in a latter stage, in keeping with the proposed progression of imaging abnormalities. Lymphangiomyomatosis (LAM) is an important differential diagnosis to pulmonary LCH. The cysts in LCH are usually more variable in size and wall thickness compared to LAM. They also show upper zone predominance compared with a diffuse involvement without zonal predominance in LAM. Lung nodule is not a typical feature in LAM. Another important distinguishing feature is that LAM occurs almost exclusively in women while LCH shows a male predominance. The final diagnosis of LCH usually relies on lung biopsy. Smoking cessation usually leads to stabilization of symptoms in majority of patients. Corticosteroid has also been demonstrated to have beneficial effect in disease stabilization or even clinical and radiological improvement. For patients with advanced pulmonary insufficiency, lung transplant has been performed with success yet recurrence of pulmonary LCH after transplant has been reported in a significant proportion of patients.
|
||
PREVIOUS CASES |
||
HOME |
COMMENTS |
|