|

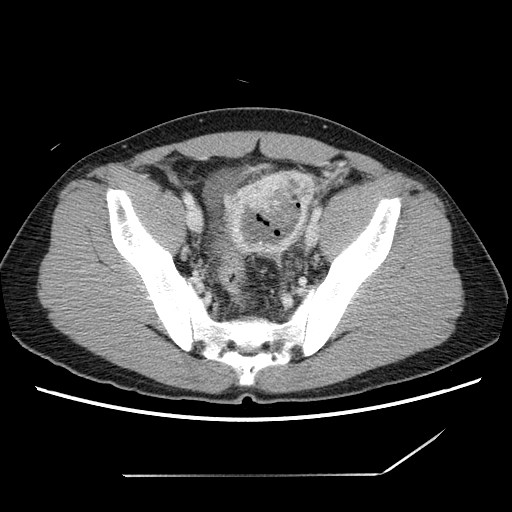

CLINICAL HISTORY: 37 year man repeatedly admitted for tarry stool required multiple transfusions. He is afebrile. Physical examination reviewed a LLQ mass. OGD and colonoscopy performed showed no significant abnormality. CT abdomen and pelvis was performed DIAGNOSIS:GIST DISCUSSION:In this patient, there is a 5.5cm x 5.3cm x 7.7cm thick walled rim enhancing lesion with cystic content and gas pockets at lower abdomen. It probably arises from the ileum. Linear calcification is evident. It is supplied by branches of SMA. Features are suggestive of tumor. There is no local invasion of surrounding structures. No evidence of intestinal obstruction. The lesion was resected and pathology came back to be GIST. GIST can occur anywhere along the GI tract. Stomach and small bowels are the commonest sites. It can also arise from peritoneum. It is associated with NF type I. It can invade adjacent organs or spread to liver. Lymphadenopathy is NOT a feature. Ulceration and fistulization to GI lumen is a common feature. In CT, it demonstrates peripheral enhancement in 92%. Central necrosis and cavity containing gas/fluid are common. It is calcified in 3%. It rarely causes intestinal obstruction. |
||
PREVIOUS CASES |
||
HOME |
COMMENTS |
|